Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250017. https://doi.org/10.20900/agmr20250017

Occupational Therapy, Health and Social Sciences Cluster, Singapore Institute of Technology, Singapore 828608, Singapore
Background: Frailty in older adults is associated with increased risks of falls, disability, and reduced quality of life. While multicomponent, community-based interventions are internationally recommended, local evidence remains limited. A recent cluster-randomised controlled trial (c-RCT) showed that the “Say No To Frailty” (SNTF) program significantly improved frailty status, physical function, and quality of life over 12 months, regardless of facilitator background. The 12-week SNTF program integrates health education, strength and balance exercises, and individual goal setting. It is delivered in groups by both healthcare and trained non-healthcare facilitators.
Methods: This case study highlights the impact of the SNTF program on behavioural change and functional outcomes in a community-dwelling older adult, Mdm V, in Singapore.
Results: Mdm V, a 76-year-old woman classified as “vulnerable” (CFS 4), joined a group led by a recently retired volunteer trained under the SNTF framework. Mdm V demonstrated meaningful improvements. Her CFS score improved from 4 to 3. Physical function increased: SPPB rose from 10 to 12; left and right grip strength improved from 12 kg to 18 kg and 10 kg to 16 kg, respectively. Knee pain reduced (EQ-5D-5L pain score: 2 to 1), and FES-I score dropped from 29 (high concern) to 18 (low concern). Her Life-Space Assessment (LSA) score rose from 72 to 82, and her self-rated health improved from 95 to 99.
Conclusions: This case demonstrates the effectiveness of SNTF in empowering older adults to achieve functional and psychosocial gains. Its success supports broader implementation in community settings as part of Singapore’s frailty strategy.
The global ageing population presents mounting challenges to public health systems, with frailty emerging as a key geriatric syndrome associated with heightened risks of falls, disability, hospitalisation, and mortality. Globally, frailty affects an estimated 10–15% of older adults [1]. In Singapore, recent data indicate that 6.2% of individuals aged 65 and above are frail, while 37% are classified as pre-frail [2]. These figures underscore the urgent need for effective, evidence-based interventions to address frailty in community-dwelling older adults.
International guidelines such as the Asia-Pacific Clinical Practice Guidelines for Frailty Management [3] and the International Conference on Frailty and Sarcopenia Research (ICFSR) guidelines [4] advocate for multicomponent interventions that target modifiable risk factors, including physical inactivity, poor nutrition, and social isolation, as a means to prevent, delay, or reverse frailty.
In Singapore, several community initiatives such as the HAPPY program, Share-A-Pot, and Gym Tonic have been implemented to promote healthy ageing [5,6]. However, these programs typically focus on single or dual components, such as exercise or nutrition, and there remains a lack of local evidence supporting comprehensive, multicomponent approaches. The SNTF program [7] seeks to fill this gap by offering a structured, group-based intervention that combines health education, progressive strength and balance exercises, and individualised goal setting to empower older adults toward sustained behavioural change. Recent findings from a c-RCT demonstrate the SNTF program’s effectiveness in improving frailty status, physical function, self-efficacy, and quality of life over 12 months, irrespective of the facilitator’s professional background [8,9].
This case study highlights the behavioural and health improvements experienced by one older adult who participated in a 12-week SNTF program conducted by a recently retired trained volunteer at an Active Ageing Centre in Singapore. It illustrates how community-based and multicomponent interventions can support positive lifestyle changes and promote healthy ageing among older adults with or at risk of frailty.
SNTF is a multicomponent group intervention designed for community-living older adults with signs of frailty and pre-frailty (Clinical Frailty Scale (CFS) scored between 4 and 6) [7]. The 12-week program integrated multidisciplinary education and physical activity in each session, comprising a 1-h pre-recorded health education segment on various topics (e.g., self-risk identification, healthy eating, home and community safety, energy conservation technique, and medication management), a 15-minute social break, and 45 mins of low-to-moderate intensity strength and balance exercises. Participants set individual goals in week 1, which were reviewed in weeks 6 and 12. Homework tasks reinforce session content and are reviewed weekly. A booster session one month post-intervention reviews learning, barriers, and strategies, while a phone follow-up at three months assesses ongoing implementation and goal attainment.
Any healthcare professionals, care workers without healthcare training backgrounds, and volunteers who have worked with older adults are eligible to attend a 2-day training course to become certified program facilitators. The program facilitator plays a key role in facilitating individuals’ learning and improving their compliance with the prescribed homework. The program uses adult learning principles [10] to allow individuals in small groups to learn the right exercises and strategies for managing different risk factors at their own pace and be responsible for their health and safety.
Outcome Measures Primary OutcomeFrailty status was assessed using the CFS, a 9-point scale ranging from 1 (very fit) to 9 (terminally ill) [11].
Secondary OutcomesPhysical function was measured using bilateral handgrip strength (average of three trials per hand) and the Short Physical Performance Battery (SPPB), which includes balance, gait speed, and chair-stand tests (maximum score = 12) [12].
Self-efficacy was evaluated using the 16-item Falls-Efficacy Scale-International (FES-I), with higher scores indicating greater fear of falling [13].
Community participation was assessed via the LSA [14], reflecting the extent, frequency, and independence of mobility. Goal attainment was measured using the Goal Attainment Scale (GAS), where participants identified and rated progress toward personal goals [15].
Quality of life was measured using the EQ-5D-5L, covering five domains (Mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and an overall health rating using a visual analogue scale (VAS) [16].
Participants’ Inclusion CriteriaParticipants were eligible if they were aged 60 years or older, living in the community, able to walk independently for more than 10 metres, and had a CFS score between 4 (vulnerable) and 6 (moderately frail). Additional criteria included an Abbreviated Mental Test (AMT) score above 5 (indicating no severe cognitive impairment) [17], no significant hearing or visual impairments, and the ability to communicate verbally in English and/or Mandarin.
Mdm V is a 69-year-old Chinese woman with secondary education. She was wearing a step tracker issued by the Health Promotion Board, Singapore. She was diagnosed with hypertension that is well-controlled with the prescribed medication.
She signed up for the SNTF program in a nearby active ageing centre in northern Singapore in March 2025. At the baseline, she experienced lethargy with a CFS score of 4 (pre-frailty), low confidence (FES-I = 29), and reduced mobility space in the community (LSA = 72). Eight other older adult participants who met the inclusion criteria joined the same program.
During the personal goal setting, she shared that, by the end of the 12-week SNTF program, she would like to: (1) reduce knee pain from 4/10 to 0/10; (2) walk for more than 30 mins without resting in between; and (3) visit her mother, who lives in another town, twice a week.
About the Program FacilitatorThe program was led by Mdm S, a recently retired volunteer in her 60s, who had completed the 2-day SNTF facilitator training workshop within three months prior to its commencement.
Pre-Post Outcome MeasuresFollowing the 12-week SNTF program, Mdm V demonstrated notable improvements across multiple domains. As shown in Figures 1 and 2, her physical function improved, with her SPPB score increasing from 10 to 12. Grip strength increased from 12 kg to 18 kg in the left hand and from 10 kg to 16 kg in the right hand. She also reported reduced knee pain, with her EQ-5D-5L pain score improving from 2 to 1. Her frailty status improved from “vulnerable” (CFS 4) to “managing well” (CFS 3). Fall efficacy showed a significant gain, with her FES-I score decreasing from 29 (high concern) to 18 (low concern). Community participation improved, as reflected in an increase in her LSA score from 72 to 82. Additionally, her self-rated health score on the EQ-5D-5L VAS rose from 95 to 99, indicating a higher perceived level of overall well-being.
In addition, she had achieved all three goals upon the completion of the 12-week SNTF intervention. She also set another new goal, which was to travel with her family to New Zealand for a holiday.
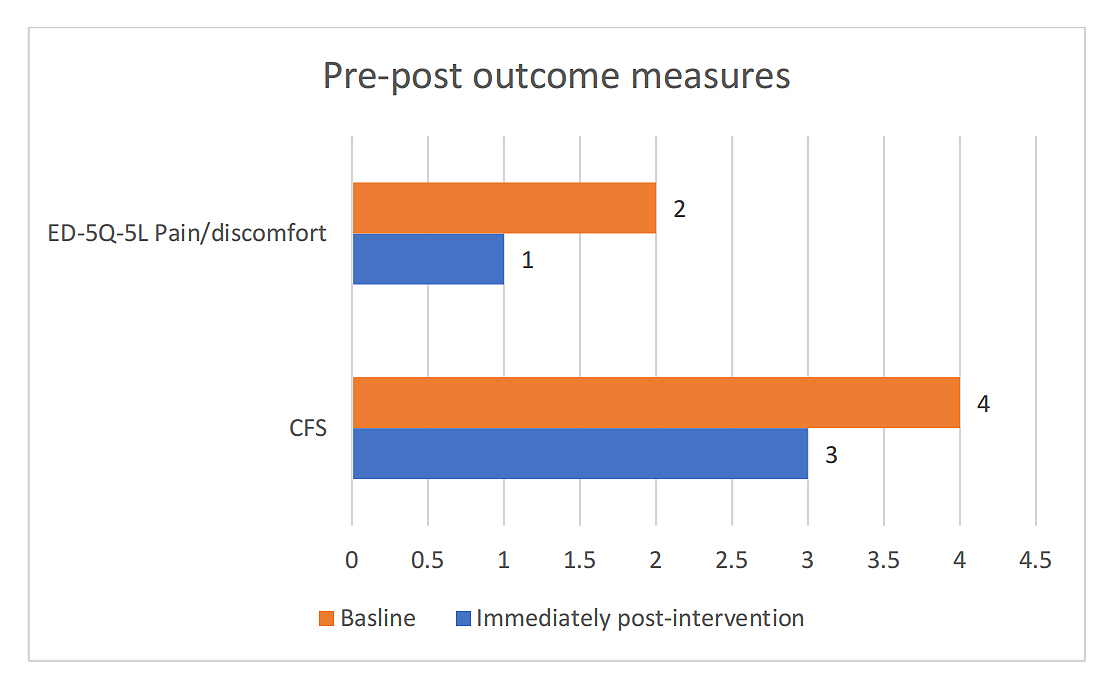 Figure 1. Pre-post outcome measure (part 1).
Figure 1. Pre-post outcome measure (part 1).
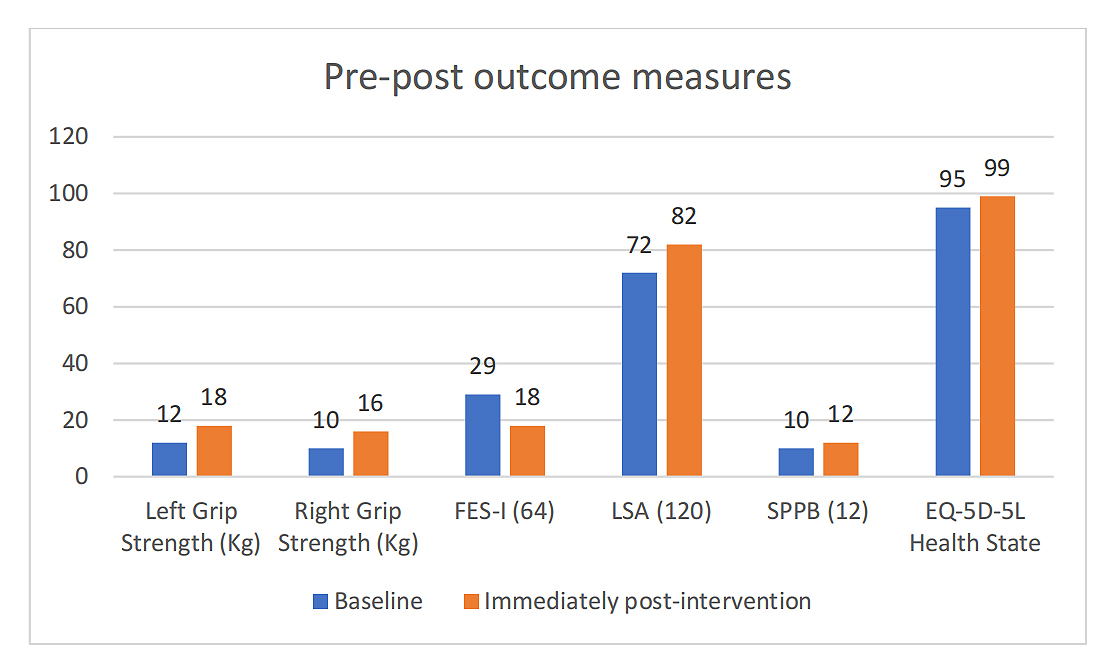 Figure 2. Pre-post outcome measure (part 2).
Figure 2. Pre-post outcome measure (part 2).
This case study of Mdm V illustrates how a multicomponent, community-based intervention such as the SNTF program can drive meaningful behavioural change and health improvements among older adults with frailty and pre-frailty. The SNTF program aligns with international guidelines [3,4] by addressing frailty through integrated strategies encompassing health education and progressive exercises with resistance components. Mdm V’s successful outcome was supported by key program components, including SMART goal setting, peer support, and regular facilitator-led engagement, which align closely with the mechanisms identified in the earlier c-RCT [7,8], where these same elements were associated with significant improvements in frailty status, physical function, and quality of life across intervention sites [8]. High adherence (95% attendance) and sustained improvements in frailty status and community participation [9] reinforce the program’s potential for wider implementation under Singapore’s National Frailty Strategy [18].
The significant reduction in Mdm V’s knee pain further highlights the therapeutic value of the SNTF program. The exercise component of the program specifically targeted core and lower limb muscle groups, including those supporting the knee joints [7]. Strengthening these muscles is known to improve joint stability and reduce pain, particularly in individuals with knee osteoarthritis [19,20]. Mdm V’s improvement, from a pain score of 2 to 1 on the EQ-5D-5L, suggests that regular engagement in these targeted exercises contributed to enhanced joint function and reduced discomfort. This outcome aligns with findings from other evidence-based exercise programs, such as the GLA:D® [21] and Otago Exercise Program [22], which recommend lower limb strengthening as an effective strategy for managing knee osteoarthritis. The inclusion of such evidence-informed exercises within the SNTF framework reinforces its clinical relevance and potential to address common musculoskeletal concerns among older adults living with frailty.
Intrinsic motivation emerged as a central driver of successful engagement in the SNTF program. The process of setting SMART goals, such as Mdm V’s goal to visit family, transformed general health messages into personally relevant objectives, promoting a deeper sense of purpose. According to Self-Determination Theory [23], autonomy, competence, and relatedness are critical to intrinsic motivation. The SNTF program’s emphasis on participant-driven goals, progress tracking, and peer interaction supported these motivational constructs. In particular, regular feedback helped participants perceive their competence, while group participation fostered a sense of connection and accountability that contributed to long-term behaviour change.
Program facilitators played a pivotal role in shaping participants’ motivational experiences. Beyond delivering content, they served as behavioural change agents who applied adult learning principles to effectively engage older adults. These principles included drawing on participants’ lived experiences, promoting active participation, and relating content to real-life situations, all of which enhanced the relevance and perceived value of the sessions. For example, Mdm V’s facilitator used empathetic and responsive communication to create a supportive environment that sustained her engagement throughout the 12-week program. Additionally, Mdm V gained confidence through repeated mastery experiences during weekly practice sessions, consistent with Bandura’s Social Cognitive Theory [24], which emphasizes self-efficacy as a key driver of behaviour change. Notably, the facilitator leading Mdm V’s group, Mdm S, was a recently retired volunteer without a healthcare background, yet she successfully guided participants through the program. This aligns with findings from other community-based interventions [5,25], which show that trained lay facilitators can effectively deliver health programs and support behavioural change, further supporting the scalability of the SNTF program.
The group-based nature of SNTF also created a platform for peer learning and social reinforcement, which is known to support behavioural adherence in older adults. Structured discussions allowed participants to share strategies, reflect on progress, and celebrate successes, fostering a sense of shared purpose and normalising setbacks. Similar to other evidence-based group interventions [26,27], these group dynamics not only encouraged regular attendance but also supported homework completion and application of learned strategies at home. For Mdm V, this social dimension was essential in maintaining both engagement and accountability over the 12-week intervention.
Notably, the successful delivery of the SNTF program by both allied health and non-healthcare facilitators [7,8] underscores its scalability across diverse community settings. The facilitator training, conducted by a master trainer, equipped individuals from varied professional backgrounds with essential competencies in communication, motivational interviewing, and behaviour change strategies. The program’s consistent outcomes across sites suggest that these skills can be reliably transferred, enabling facilitators without clinical training to lead sessions effectively. However, a key barrier to wider implementation has been the shortage of manpower in active ageing centres in Singapore. To address this, the research team recruited community volunteers, such as Mdm S, and provided them with a structured 2-day training to build their group facilitation skills. Expanding this pool of trained volunteers offers a practical and sustainable strategy for scaling the SNTF program across more centres, thereby enhancing its reach and impact.
While the studied intervention was part of the most recent implementation in 2025, no follow-up data were collected for this group. However, long-term findings [8] from the larger clinical trial [7] suggest that the SNTF program supports sustained behavioural change, with improvements in physical function, frailty status, and community participation maintained up to 9 months post-intervention. Several program features likely contributed to this durability, including SMART goal-setting, which linked health behaviours to personally meaningful outcomes, and weekly home-based tasks that reinforced habit formation. These components are also commonly embedded in other evidence-based community programs targeting chronic disease management [27] and fall prevention [26]. Additionally, group-based peer support promoted accountability and motivation, while the booster session and follow-up calls offered continued reinforcement. Collectively, these elements reflect established strategies for sustaining behaviour change and underscore the program’s potential effectiveness beyond the initial intervention period.
This report presents a single case study, and as such, several limitations must be acknowledged. First, the absence of statistical analysis limits the ability to draw broader conclusions about program efficacy. The pre-post comparisons, while informative, are descriptive in nature and cannot establish causality. Second, long-term outcomes remain unknown, as the program at this participating centre concluded only recently in June 2025. Follow-up data would be needed to evaluate whether the observed improvements in physical function, frailty status, and community participation are sustained over time. Third, given the individualised nature of this case and the specific context in which the intervention was delivered, the findings may not be generalisable to other populations or settings. Nevertheless, this case provides valuable insights into the lived experience of an older adult undergoing a structured community-based frailty program and highlights key mechanisms, such as intrinsic motivation and facilitator support. The clinical effectiveness of the intervention will be revealed from our larger clinical trial.
This case highlights the critical role of intrinsic motivation, peer support, and competent facilitation in effective community-based frailty management. The SNTF program demonstrates that a multicomponent, group-based approach can lead to meaningful functional and psychosocial gains among older adults. As the program scales across diverse community settings, careful selection and training of facilitators, regardless of training background, will be essential to maintaining program effectiveness and ensuring sustainability at the population level.
This case study is part of the wider implementation study. The clinical trial protocol has been registered with the Australian New Zealand Clinical Trials Registry (ACTRN12624000908538p).
The study was approved by the Institutional Review Board of Singapore Institute of Technology (RECAS-0409, 21 August 2024) for studies involving humans. Informed consent was obtained from all subjects involved in the study.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The dataset of the study is available from the corresponding author upon reasonable request.
The author declares that he has no conflicts of interest.
This study did not receive any external funding.
The author would like to thank all program facilitators and participants who participated in this study.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
Xu T. Facilitating positive behavioural change in community-dwelling older adults with frailty: A case study in singapore. Adv Geriatr Med Res. 2025;7(3):e250017. https://doi.org/10.20900/agmr20250017.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




