Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(1): e260002. https://doi.org/10.20900/agmr20260002
 ,
Edward Nasco 1,2 ,
Noel Lorenzo-Villalba 1,2
,
Edward Nasco 1,2 ,
Noel Lorenzo-Villalba 1,2
1 Department of Internal Medicine, Hôpital de Hautepierre, University Hospital of Strasbourg, 67000 Strasbourg, France.
2 Competence Center for Autoimmune Cytopenias (Cereal), University Hospitals of Strasbourg (HUS), Strasbourg, France
* Correspondence: Emmanuel Andrès
Primary immune thrombocytopenia (ITP) is entering a new era shaped by precision medicine, digital health, and geroscience, with key implications for patients ≥65 years. In this population, therapy balances efficacy with minimizing systemic toxicity and age-related complications. Corticosteroids are used cautiously due to metabolic, infectious, and neuropsychiatric risks, while thrombopoietin receptor agonists (TPO-RAs) have become preferred for long-term management. Individualized targets (~50–100 ×109/L) aim to ensure hemostasis while limiting thrombotic risk. Advances in immunogenetics, transcriptomics, and pharmacogenomics improve patient stratification and prediction of treatment response and relapse. Artificial intelligence and Big Data applied to integrated clinical and omics datasets support diagnosis, risk modeling, and personalized therapy sequencing. Geriatric-specific assessment—including frailty, fall risk, polypharmacy, cognition, and adherence—combined with digital longitudinal monitoring, enhances preventive care. These innovations underpin the concept of geriatric–immune systemic ITP (G-ITP), framing ITP in older adults as a systemic disorder influenced by immunosenescence, clonal hematopoiesis, endothelial dysfunction, and frailty rather than isolated autoimmunity. Integrating comprehensive geriatric assessment with personalized TPO-RA therapy may improve outcomes and reduce morbidity, establishing ITP as a model for geroscience-informed, patient-centered immune care.
Primary immune thrombocytopenia (ITP) is a rare, acquired autoimmune disorder defined by isolated thrombocytopenia (platelet count <100 × 109/L [100 /mm3]), predominantly caused by autoantibody-mediated peripheral platelet destruction [1]. Historically regarded as a diagnosis of exclusion and managed empirically, ITP has long posed substantial challenges in diagnostic evaluation and therapeutic decision-making. Over recent decades, however, advances in biology and digital technologies have progressively reshaped both the conceptual framework and clinical management of the disease.
Developments in molecular biology have enabled the identification of immunogenetic alterations, transcriptomic signatures, and immune biomarkers, improving patient stratification and facilitating differentiation between primary ITP, secondary thrombocytopenias, and syndromic immune-mediated cytopenias [2]. In parallel, Artificial Intelligence (AI)–based and predictive modelling approaches allow integration of multidimensional clinical, biological, and omics datasets to estimate disease trajectory, treatment response, and relapse risk, supporting a transition from reactive to anticipatory care. The expansion of Big Data resources—including registries, biobanks, and multi-omics platforms—has further provided real-world insights into rare phenotypes, therapeutic patterns, and long-term outcomes.
Digital health innovations, such as telemedicine and longitudinal remote monitoring, are increasingly incorporated into routine care, enabling assessment of clinical evolution, treatment adherence, and tolerability beyond traditional clinical settings. These strategies are particularly relevant in chronic disease management and in geographically underserved populations.
Collectively, these advances underpin a shift from population-based treatment algorithms toward individualized and patient-centered care. This evolution is especially pertinent in older adults, who face specific challenges related to multimorbidity, polypharmacy, immuno-senescence, and frailty [3,4]. These factors modify disease presentation, influence treatment tolerability, and affect clinical outcomes. Within this context, the emerging geriatric–immune systemic ITP (G-ITP) paradigm conceptualizes ITP in older adults as a systemic condition shaped by age-related immune dysfunction and biological vulnerability, rather than as an isolated autoimmune cytopenia.
This review critically examines the impact of these technological and biological advances on the diagnosis, management, and prognosis of ITP, with particular emphasis on the challenges and unmet needs of an increasingly complex and ageing patient population.
Specificities in Diagnosis And Management of itp in Elderly PatientsOlder adults (commonly defined as ≥65 years) constitute a distinct and clinically challenging subgroup of patients with ITP, characterized by greater disease complexity, a higher burden of comorbidities, and a critical need for risk-mitigation strategies. From a prognostic perspective, ITP in this population is associated with a substantially increased mortality risk, driven predominantly by severe infections and cardiovascular events rather than bleeding itself [3]. Diagnostic evaluation also differs from that in younger patients: the threshold for bone marrow examination is lower owing to the increased prevalence of secondary causes of thrombocytopenia, particularly myelodysplastic syndromes and drug-induced thrombocytopenia in the setting of polypharmacy.
Management in older patients must prioritize minimization of treatment-related toxicity. Corticosteroids, although effective, should be prescribed at the lowest effective dose and for the shortest possible duration because of the high risk of adverse effects, including delirium, infection, and metabolic decompensation [4]. Intravenous immunoglobulins (IVIgs) remains a valuable option for rapid platelet elevation, but careful monitoring is required to avoid complications related to fluid overload and renal dysfunction.
Thrombopoietin receptor agonists (TPO-RAs) have emerged as the preferred maintenance therapy in older adults, with response rates comparable to those observed in younger populations (approximately 60–80%) [5]. Their use, however, requires careful dose titration and close monitoring because of the intrinsically higher, age-associated thrombotic risk. Treatment strategies should aim for lower platelet targets (approximately 50–100 × 109/L) and avoid excessive platelet responses (>400 × 109/L) [5]. Lower starting doses with gradual escalation are recommended to account for age-related changes in hepatic and renal clearance. In patients with complex polypharmacy, selection of oral TPO-RAs with limited drug–drug or drug–food interactions, such as avatrombopag, may facilitate adherence. Overall, optimal management in this population requires a personalized, multidisciplinary approach that combines rigorous exclusion of secondary causes with risk-adapted use of TPO-RAs to maintain hemostatic platelet levels while minimizing systemic toxicity and cardiovascular risk [6–9].
Conceptually, ITP in older adults should no longer be viewed as an isolated autoimmune cytopenia, but rather as a geriatric–immune systemic disorder shaped by interactions between ageing-related biological processes and immune dysregulation [4]. Immuno-senescence alters innate and adaptive immune responses, promoting chronic inflammation, impaired immune tolerance, and dysregulated autoantibody production [2]. Concurrently, age-related clonal hematopoiesis introduces additional immune and inflammatory perturbations that may influence platelet production, immune recognition, and therapeutic responsiveness [2,4]. Endothelial dysfunction and increased vascular vulnerability further modify the clinical phenotype, contributing to a distinct balance between bleeding and thrombotic risks in older patients [2]. Frailty, multimorbidity, and polypharmacy act as major modifiers of disease expression and treatment tolerance, underscoring the need for an integrated geriatric, rather than purely hematological, framework.
This reconceptualization has important diagnostic and therapeutic implications. In older adults, platelet thresholds for intervention are often lower, the risk–benefit profile of immunosuppressive strategies such as splenectomy or rituximab differs substantially, and invasive procedures are frequently avoided [4]. Treatment escalation should therefore incorporate not only platelet counts and bleeding risk but also functional status, comorbidities, cognitive reserve, and life expectancy. Within this context, conventional diagnostic algorithms and uniform treatment strategies are increasingly inadequate.
Reframing ITP in Older Adults: A Geriatric–Immune Systemic Disorder within a Geroscience and Precision Medicine FrameworkThis conceptual evolution is reinforced by recent advances in geroscience, which provide a biological framework for understanding ageing as an active and potentially modifiable determinant of disease rather than a passive background variable. In this context, the work by Jurja and colleagues (2023) offers an important peer-reviewed illustration of geroscience principles, demonstrating that ageing-related biological processes can be therapeutically targeted to modify disease trajectories and functional outcomes [10]. Although focused on retinal health and xanthophyll supplementation, this study underscores a broader concept that is directly applicable to ITP in older adults: geriatric risk is a biologically active contributor to disease phenotype and treatment response.
Applied to ITP, this perspective supports the view that age-associated immune dysregulation, endothelial vulnerability, metabolic alterations, and reduced physiological reserve actively shape both clinical presentation and therapeutic efficacy [2,4]. The geriatric–immune systemic model of ITP (G-ITP) is therefore consistent with geroscience principles, in that it recognizes the need for interventions that extend beyond correction of platelet counts to address the ageing-related biological milieu governing immune responsiveness, vascular integrity, and resilience to treatment-related stressors [2]. This framework helps explain the distinct therapeutic thresholds, altered benefit–risk profiles, and heterogeneous responses to standard ITP therapies observed in older patients compared with younger adults [4].
Integration of geroscience with artificial intelligence–driven precision medicine further strengthens this approach. AI-based decision-support systems can incorporate ageing biomarkers, frailty measures, comorbidity burden, and longitudinal functional data alongside conventional hematological parameters. Such models move beyond disease-centered predictions towards biologically informed, patient-centered recommendations, translating complex ageing biology into clinically actionable insights. In doing so, AI enables anticipation of differential treatment responses, reduction of iatrogenic harm, and tailoring of therapeutic strategies according to biological rather than chronological age.
Experience of the Strasbourg’s University HospitalAt the University Hospital of Strasbourg (Hôpitaux Universitaires de Strasbourg, France), a tertiary reference center, a retrospective review was conducted of 62 patients aged >75 years with newly diagnosed ITP (personal data, partial data in [11]). The cohort exhibited a mean platelet count at diagnosis of approximately 28×109/L, with nearly half-presenting mild or absent bleeding manifestations despite profound thrombocytopenia. Comorbidities were highly prevalent: over 80% had hypertension, 45% chronic kidney disease, and more than 60% were on five or more medications, complicating management.
First‑line therapy mainly consisted of low‑dose prednisone (≤0.5 mg/kg/day) in 70% of patients and IVIgs in 25% during acute bleeding events; the initial response rate was 65%, but early relapse within 6 months occurred in 40%. Second‑line treatment with TPO‑RAs achieved a sustained response in 72% of treated patients, with a mean maintenance platelet count of 75 ×109/L and no major thromboembolic events recorded. The median follow‑up was 30 months, during which the all‑cause mortality was 22%, primarily attributed to comorbid cardiovascular disease rather than hemorrhagic complications.
Importantly, a comprehensive geriatric assessment—including frailty scoring, cognition, and polypharmacy review—was integrated into the care pathway, enabling individualized treatment adjustments and improved tolerability.
Evidence Gaps and Unmet Needs in Elderly Patients with ITPDespite the increasing prevalence of ITP in older adults, the evidence base guiding optimal management in this population remains limited. Older patients are consistently underrepresented in clinical trials, and age-specific considerations are insufficiently addressed in current guidelines, resulting in substantial unmet clinical needs [2].
Patients aged 75 years or older, or those with significant comorbidities, are frequently excluded from pivotal ITP studies [2,4]. Consequently, efficacy and safety data for commonly used therapies—including even splenectomy, TPO-RAs, rituximab, fostamatinib, and emerging agents—are largely extrapolated from younger, fitter populations. This limits the generalizability of trial findings to older adults, in whom altered pharmacokinetics, increased vulnerability to adverse events, and competing non-hemorrhagic risks are common [4].
Risk stratification represents a major gap in the management of elderly patients with ITP. Existing bleeding scores and platelet count thresholds do not adequately capture age-related modifiers such as frailty, vascular disease, atrial fibrillation, or the frequent use of antiplatelet and anticoagulant therapies. As a result, clinicians lack validated tools to balance bleeding risk against the heightened thrombotic risk characteristic of this population [4].
Comorbidities and polypharmacy further complicate treatment decisions. Older patients with ITP often require multiple long-term medications, yet potential drug–drug interactions between ITP therapies and commonly prescribed agents—such as anticoagulants, antihypertensive drugs, or antidiabetic treatments—have not been systematically evaluated [4]. The cumulative burden of polypharmacy increases the risk of toxicity, non-adherence, and premature treatment discontinuation, factors that remain under-represented in both clinical trials and real-world datasets.
Current therapeutic studies predominantly rely on platelet response as the primary endpoint, with limited consideration of outcomes that are particularly relevant to older adults, including functional status, independence, quality of life, cognitive effects, and avoidance of hospitalization [2,4]. Redefining treatment success to incorporate patient-centered and geriatric outcomes, rather than hematological response alone, is therefore an important unmet need.
Data on the long-term safety of chronic ITP therapies in older patients are sparse. Prolonged exposure raises concerns regarding sustained immunosuppression, infection risk, malignancy, hepatic toxicity, and thromboembolic complications. Moreover, evidence-based guidance on optimal treatment sequencing in this population—balancing efficacy, tolerability, and reversibility—remains largely absent [2,4].
Finally, older adults with ITP represent a highly heterogeneous population, ranging from robust individuals to those with advanced frailty [4]. Frailty assessments are rarely incorporated into clinical trials or routine decision-making, promoting uniform treatment approaches that risk both overtreatment and under treatment. Addressing these gaps will require dedicated prospective studies and real-world registries with inclusive eligibility criteria and stratification by age, frailty, and comorbidity burden. Multidisciplinary collaboration among hematologists, geriatricians, and primary care physicians will be essential to develop individualized management strategies aligned with patient goals and to improve outcomes in this growing patient population [2,4].
Molecular Biology: Towards Precise Stratification of ITPAdvances in molecular biology have provided key insights into the immuno-pathogenesis of ITP through the identification of specific immunogenetic alterations and transcriptomic signatures associated with disease development and persistence [2]. High-resolution profiling of B-cell and T-cell repertoires, together with detailed characterization of pathogenic autoantibodies targeting platelet glycoproteins such as GPIIb/IIIa, has clarified central immune effector mechanisms underlying peripheral platelet destruction [2]. In parallel, next-generation sequencing–based interrogation of the bone marrow microenvironment has revealed abnormal immune cell interactions, dysregulated cytokine signaling, and altered megakaryocyte–immune crosstalk, contributing to impaired platelet production [2].
The identification of rare germline or somatic variants affecting immune tolerance and signaling pathways, including CTLA-4, LRBA, and STAT3, has further linked a subset of ITP presentations to familial or syndromic forms of disease, frequently overlapping with primary immunodeficiency and immune dysregulation syndromes [1,2]. Together, these findings advocate for a molecularly informed classification of ITP that moves beyond the conventional view of an isolated autoimmune cytopenia, allowing more accurate distinction between primary ITP, secondary thrombocytopenias, and immune-mediated cytopenias associated with broader immunodeficiency syndromes.
Ultimately, comprehensive molecular profiling has the potential to inform personalized therapeutic strategies by identifying patients most likely to benefit from targeted immunomodulatory approaches, including inhibitors of the JAK–STAT pathway, immune checkpoint modulation, or other mechanism-based interventions, thereby advancing precision medicine in ITP management.
Predictive Medicine: Personalizing Therapeutic DecisionsPredictive medicine seeks to anticipate disease course and treatment response through the integration of individual risk factors across genetic, immunological, biological, and environmental domains. This approach is particularly relevant in ITP, given the substantial heterogeneity in clinical presentation, disease progression, and therapeutic outcomes. Predictive models combining clinical variables—such as age at diagnosis and disease subtype—with biological markers, including antiplatelet antibody status, cytokine profiles, and indicators of immune activation, as well as genetic features such as HLA polymorphisms, are increasingly able to forecast disease chronicity, relapse following first-line therapy, and failure of standard treatments [1,8]. These multidimensional approaches had better reflect the complex pathophysiology of ITP than traditional prognostic factors alone (Table 1).
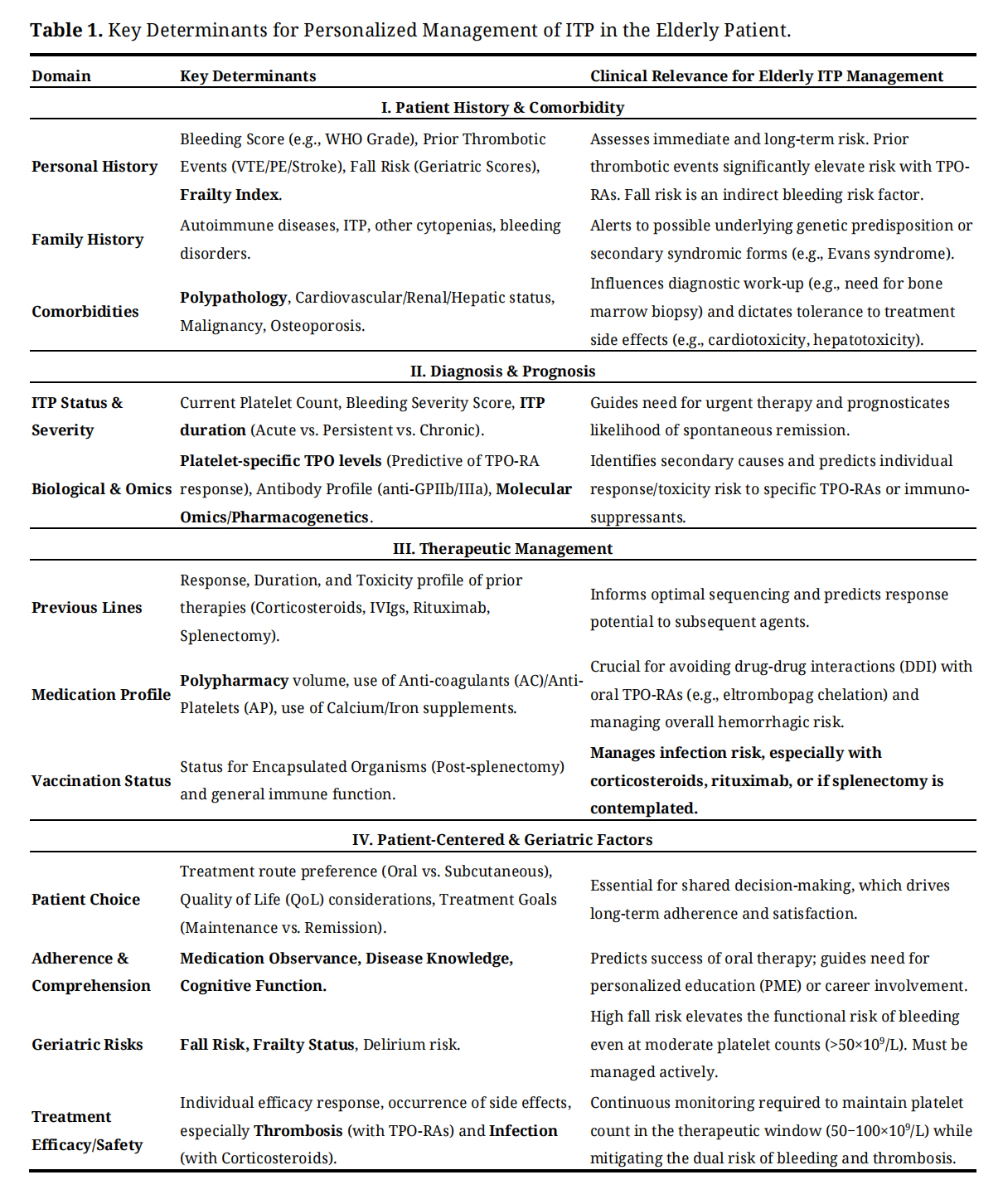 Table 1. Key Determinants for Personalized Management of ITP in the Elderly Patient.
Table 1. Key Determinants for Personalized Management of ITP in the Elderly Patient.
Integration of such predictive tools into clinical practice, increasingly supported by decision-support algorithms embedded within routine workflows, has the potential to enable genuinely individualized therapeutic strategies and to limit unnecessary exposure to prolonged or non-specific immunosuppression. Stratification of patients according to predicted disease trajectory and treatment responsiveness may allow optimization of treatment timing and sequencing. In addition, the identification of molecular and immunological signatures associated with response to thrombopoietin receptor agonists supports their earlier and more targeted use in selected patients, with the aim of maximizing efficacy while minimizing adverse events and long-term treatment burden [9]. Collectively, predictive medicine represents a key step towards precision-based management of ITP, aligning therapeutic decisions with individual biological profiles rather than population-based averages.
Preventive Medicine: Avoiding Relapses and ComplicationsPreventive approaches in ITP should move beyond reactive care, aiming to proactively mitigate relapse, severe bleeding, and both treatment-related and age-related toxicities [11]. This approach is particularly relevant in older adults, in whom disease-specific complications intersect with geriatric vulnerability. Advances in immune monitoring technologies now allow early detection of subclinical immunological changes—such as clonal T-cell expansion, alterations in regulatory T-cell populations, or increases in pro-inflammatory cytokines—that may precede clinical relapse. Recognition of these early signals creates opportunities for timely preventive interventions, including dose adjustment, treatment modification, or intensified monitoring, before overt clinical deterioration occurs [1,2].
Prevention of infectious complications remains a central component of ITP management and requires individualized assessment of vaccination status, immunoglobulin levels, and infection history, particularly in patients exposed to B-cell–depleting therapies or prolonged corticosteroid use. In older adults, preventive strategies must additionally account for multimorbidity and polypharmacy, which substantially increase the risk of adverse drug reactions and treatment discontinuation. In this context, digital longitudinal monitoring platforms are assuming an increasingly important role by integrating biological parameters with structured assessment of key geriatric risks, including medication adherence, cognitive function, and fall risk related to frailty or fluctuating platelet counts [11]. Such integrated digital approaches facilitate early identification of drug–drug interactions, support timely therapeutic adjustments, and enable delivery of tailored patient education. Collectively, these preventive strategies have the potential to improve adherence, reduce avoidable clinical decompensation, and enhance overall safety in the management of this complex and vulnerable patient population.
AI: c Diagnosis and Decision-MakingAI, including machine learning and deep learning approaches, offers a transformative opportunity to address the complexity of ITP in older adults. AI systems are particularly suited to analyzing high-dimensional, heterogeneous datasets that integrate clinical features, laboratory parameters, imaging, genomics, and longitudinal outcomes. Supervised machine learning algorithms trained on large, well-annotated clinical and biological datasets have demonstrated high diagnostic accuracy, with sensitivities and specificities exceeding 90% in distinguishing ITP from alternative causes of thrombocytopenia, including drug-induced cytopenias, bone marrow failure syndromes, and systemic autoimmune diseases [11]. Such tools are especially valuable in older patients, in whom overlapping etiologies and atypical presentations are common.
Beyond diagnosis, AI-based predictive models can forecast individual responses to corticosteroids, IVIgs, TPO-RAs, and other therapies [4]. By simultaneously evaluating thousands of clinical, molecular, and biological variables, these models can identify patient-specific response patterns, estimate relapse risk, and anticipate treatment-related adverse events. This capability is particularly relevant in geriatric ITP, where minimizing toxicity and avoiding overtreatment are central objectives. AI-driven decision support systems also have potential to optimize treatment sequencing, adjust dose intensity, and identify patients who may benefit from early alternative strategies.
Integration of AI into electronic health records could, in the near future, provide real-time, personalized recommendations at the point of care. Such systems may assist clinicians in balancing bleeding and thrombotic risks, refining therapeutic thresholds, and standardizing care while preserving individualized decision-making. Importantly, this approach aligns with broader geroscience and precision medicine paradigms, recognizing ageing as a biologically active determinant of disease phenotype and treatment response. Embedded within a geriatric–immune conceptual framework, AI has the potential to support a more precise, equitable, and biologically informed model of ITP management in older adults [4,11].
Big Data: Harnessing Massive Datasets for Better Understanding and TreatmentThe application of Big Data in ITP constitutes a major clinical and scientific advance, enabling the integrated analysis of large-scale datasets derived from national registries, prospective cohorts, hospital information systems, biobanks, and multi-omics platforms, including genomics and proteomics. Once harmonized and standardized, these heterogeneous data sources can be interrogated using advanced statistical methods and AI-based algorithms, facilitating the identification of rare or previously unrecognized clinical phenotypes, the discovery of novel biomarkers predictive of treatment response or toxicity, and the generation of new pathophysiological hypotheses that extend beyond conventional disease models [8,11]. This approach is particularly relevant in ITP, where clinical heterogeneity and variable treatment responses limit the applicability of traditional trial-based evidence.
Real-world Big Data analyses have already demonstrated clinical utility by identifying patient subsets who respond to TPO-RAs and can be safely maintained on reduced doses, supporting individualized tapering strategies and minimizing long-term exposure and toxicity. Integration of longitudinal clinical data with high-throughput sequencing further allows identification of multifactorial molecular and immunological signatures associated with progression from acute to chronic ITP, providing insights into mechanisms of disease persistence. Beyond individual patient management, Big Data approaches substantially enhance pharmaco-epidemiological research, enabling near real-time evaluation of the effectiveness, safety, and healthcare impact of emerging biologic therapies across diverse populations. The granularity of such analyses—capturing morbidity, hospitalization rates, and long-term outcomes—exceeds that achievable in conventional randomized trials, supporting ongoing refinement of therapeutic strategies in routine clinical practice [11].
Telemedicine: Personalized and Secure Remote MonitoringTelemedicine offers an innovative, secure, and patient-centered approach for the longitudinal management of ITP, particularly in chronic cases, patients in remote locations, or during public health emergencies. Secure digital platforms enable remote consultations, allowing clinicians to assess disease evolution in real time, review laboratory results, discuss adverse effects, and adjust treatment without the need for in-person visits [11,12]. The integration of connected monitoring technologies—including symptom-reporting applications, remote platelet counters, and wearable sensors—enhances outpatient safety by facilitating continuous surveillance and early detection of clinical deterioration, thereby reducing unnecessary hospital visits and exposure to healthcare-associated risks.
Telemedicine also supports remote delivery of personalized therapeutic education, promoting patient engagement, adherence, and autonomy. This participatory model is particularly relevant in ITP, where disease unpredictability and bleeding-related anxiety necessitate frequent communication and reassurance [11,12]. Future developments are expected to integrate telemedicine platforms with hospital electronic health records, laboratory information systems, and AI-driven decision-support tools, creating a seamless ecosystem capable of generating individualized, real-time recommendations. Such integration has the potential to advance precision medicine in ITP, optimize resource utilization, and improve both clinical outcomes and patient-reported experiences [11].
ITP is entering a transformative era, driven by technological and biological advances that are reshaping hematology and patient care. Molecular profiling now enables precise patient stratification through identification of immunogenetic alterations, transcriptomic signatures, and predictive biomarkers, while predictive medicine allows anticipation of disease trajectory, therapeutic response, and relapse risk. Preventive strategies, particularly in older adults, optimize management of bleeding complications, treatment-related toxicities, and geriatric vulnerabilities, including frailty, comorbidities, and polypharmacy. Artificial intelligence supports clinical decision-making by integrating multidimensional datasets to generate individualized, real-time recommendations, while Big Data approaches—drawing from national registries, biobanks, multi-omics platforms, and real-world evidence—reveal rare clinical phenotypes, novel therapeutic targets, and long-term outcomes. Telemedicine complements these innovations by enabling secure, patient-centered remote follow-up, continuous monitoring, education, and participatory care, particularly for vulnerable or geographically distant patients [11,12].
The emergence of the geriatric–immune systemic ITP (G-ITP) paradigm highlights that, in older adults, ITP should be viewed not as an isolated autoimmune cytopenia but as a systemic disorder shaped by immuno-senescence, clonal hematopoiesis, endothelial dysfunction, and frailty. Integrating G-ITP principles with precision medicine tools allows clinicians to tailor interventions not only to platelet counts but also to biological age, functional reserve, and overall risk profile. The convergence of molecular profiling, predictive modelling, AI-supported analytics, Big Data, telemedicine, and geroscience insights establishes a proactive, synergistic framework capable of addressing the complexity of ITP, improving outcomes, and respecting patient individuality.
Realizing the full potential of this model will require interoperable digital systems, robust data quality and security, and specialized training for healthcare professionals in advanced analytic and monitoring technologies. Longitudinal studies incorporating geroscience metrics, real-world evidence, and patient-reported outcomes will be essential to refine the G-ITP framework and validate personalized intervention strategies. In this evolving landscape, ITP serves as a paradigm not only for the application of cutting-edge technology in hematology but also for the broader implementation of personalized, human-centered, and geroscience-informed care, demonstrating how age-modulated immune disorders can be managed with precision, safety, and efficacy.
In accordance with current regulations, retrospective observational studies based on routinely collected, fully anonymized clinical data do not require approval from an ethics committee nor specific informed consent from patients.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
All data generated from the study are available in the manuscript.
The authors declare that they have contributed equally to all stages of the manuscript's preparation. Specifically, EA, EN and NL-V participated in the conceptualization, literature review, drafting, critical revision, and final approval of this text. Both authors are accountable for all aspects of the work.
The authors declare having received honoraria, research grants, and/or non-financial support from pharmaceutical companies marketing Thrombopoietin Receptor Agonists for immune thrombocytopenia, including AMGEN, Pfizer and GSK. This support was received for activities such as consulting, serving on advisory boards, speaking at scientific events, and/or participating as an investigator in clinical trials. However, the author(s) affirm that these financial relationships did not influence the design, conduct, data analysis, or interpretation of the results and conclusions presented in this article.
None.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Andrès E, Nasco E, Lorenzo-Villalba N. Primary Immune Thrombocytopenia in Elderly Patients in the Era of Emerging Technologies: Towards an Integrated and Personalized Medicine. Adv Geriatr Med Res. 2026;8(1):e260002. https://doi.org/10.20900/agmr20260002.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




