Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(1):e260003. https://doi.org/10.20900/agmr20260003
 ,
Isabel Lorenzo 3 ,
Elisabet Palomera 1 ,
Jessica Martínez 4 ,
Marta Cuquet 5 ,
Emili Burdoy 6 ,
Eulogio Pleguezuelos 7 ,
Mateu Cabré 8
,
Isabel Lorenzo 3 ,
Elisabet Palomera 1 ,
Jessica Martínez 4 ,
Marta Cuquet 5 ,
Emili Burdoy 6 ,
Eulogio Pleguezuelos 7 ,
Mateu Cabré 8
1 Research Unit, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
2 Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHD), Instituto de Salud Carlos III, 28029 Madrid, Spain
3 Information Management Unit, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
4 Dietetics and Nutritional Unit, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
5 Tecnocampus Foundation, 08302 Mataró, Barcelona, Spain
6 Primary Care Department, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
7 Rehabilitation Department, Hospital de Mataró, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
8 Internal Medicine Department, Consorci Sanitari del Maresme, 08304 Mataró, Barcelona, Spain
* Correspondence: Mateu Serra-Prat
Background: Low-grade chronic dehydration may have mid-to-long-term effects on muscle function. Objectives: To assess hydration status and intracellular hydration of right-leg lean mass for a community-dwelling aged population, and to assess the relationship with thigh muscle function decline. Methods: Design: observational prospective study of individuals aged ≥70 years followed up for 12 months. Measures: body composition and hydration status were assessed by bioelectrical impedance analysis (BIA) and isokinetic testing was used to measure right-knee flexion and extension strength, work, and power. The intracellular water/fat free-mass ratio (ICW/FFM) was considered the main study factor. Results: Of 117 recruited individuals (75.0 ± 4.1 years, 50.4% women), 52 were available for 12-month follow-up. After adjusting for age, sex, and number of medications, right-leg ICW/FFM showed an independent effect on 12-month increases in right-leg extension strength (beta = 1120 N, p = 0.078), work (beta = 2356 J, p = 0.017), and power (beta = 1921 W, p = 0.021), and in flexion strength (beta = 1610 N, p = 0.134), work (beta = 6270 J, p = 0.008), and power (beta = 5183 W, p = 0.003). Conclusions: BIA indicators of poor lower-limb muscle hydration are correlated with a decline in certain muscle function parameters in the same limb, suggesting that dehydration may affect muscle function in aged populations.
Water represents approximately two thirds of the body weight of young adults [1]. This percentage progressively declines with age, mainly because of a relative decrease in fat-free mass (FFM) and muscle mass, but also because of low-grade chronic dehydration in aged individuals [2]. This dehydration may be the result of poor water intake (due to a reduced thirst sensation, dysphagia, or a fear of urinary incontinence) or increased water loss due to medication (such as diuretics or laxatives) or physiological changes associated with ageing (such as kidney failure or peripheral resistance to arginine-vasopressin) [3,4]. Chronic dehydration, which occurs in approximately 20–30% of older adults, leads to increased risks of morbidity, disability, and mortality [5]. While dehydration in young athletes has been associated with inflammation [6], metabolic, kidney, and cardiovascular impairments [7], and muscular weakness [8], its relationship with muscle function in the aged population has less well understood.
Water flows between intracellular and extracellular compartments, balancing osmolarity in both sides of the cell membrane. Hyperosmotic stress, which reflects increased extracellular osmolarity, leads to cell dehydration and damage [9]. Ageing leads to a decrease in muscle cell mass and a relative expansion of extracellular water (ECW) [10], both associated with poor muscle strength and decreased gait speed in older individuals [10–12]. Similarly, the ratio of intracellular water (ICW) to total water (TW) in the lower limbs has been shown to be a predictor of dorsiflexion and plantar flexion strength [13], while the ICW/FFM ratio (an indicator of intracellular hydration and muscle quality measured in L/kg) has been linked to poor muscle strength, impaired functional capacity, and greater frailty risk [14,15].
However, these preliminary results need to be corroborated, both in prospective studies with more accurate measurements of body composition and muscle function and in studies of the same specific muscle groups. A cross-sectional study assessing both hydration and muscle function in the same lower-limb muscle group has shown that the right-leg ICW/FFM ratio is not correlated with right-knee muscle flexion and extension strength, work, or power, but with sarcopenia and dynapenia in women and with timed up-and-go (TUG) test results in men [16]. In the aged population, both muscle function and physical performance decline are poorly understood, and since low-grade chronic dehydration may have long-term effects on muscle function, further research is required, most especially longitudinal studies that assess the predictive value of dehydration indicators.
The aim of this study, conducted in a community-dwelling aged population, was to assess the effect of whole-body and right-leg hydration status on right-knee muscle flexion and extension function. As secondary aims we evaluated changes in hydration status and right-knee muscle function over a period of 12 months in the same population.
An observational prospective study with 12-month follow-up was conducted of community-dwelling individuals aged ≥70 years. Individuals randomly selected from the database of inhabitants ascribed to 3 primary care centres in the Maresme region (Catalonia, Spain) were invited by telephone to participate. If they agreed, a screening visit was arranged with their primary care physician to check eligibility criteria, deliver information on the study, and obtain their signed consent. Excluded were individuals unable to do the isokinetic test (due to injuries, wounds, etc.), with active malignancy, neuromuscular disease, bilateral knee or hip prostheses, dementia, serious mental illness, life expectancy <6 months, and in palliative care or institutionalized. Baseline evaluation took place between June and November 2021 and follow-up continued until January 2023. The local ethics committee approved the study protocol (code CEIm 65/19).
Data CollectionData collected in the baseline visit, which included a physical examination, were as follows: sociodemographic characteristics (age, sex); comorbidities (osteoarthritis or rheumatism, ischaemic heart disease or heart failure, peripheral vascular disease, stroke, depression, previous resolved cancer history, chronic bronchitis or chronic obstructive pulmonary disease, asthma, diabetes, gastroduodenal ulcer, gastroesophageal reflux disease, chronic liver disease, chronic kidney failure, hypertension, dyslipidaemia); chronic medication use; and weight, height, and body mass index (BMI). Data was obtained directly from patient interviews and physical examinations and from primary care electronic clinical records. Evaluated in both the baseline and 12-month follow-up visits were hydration status, muscle function, functional capacity, and physical performance.
Hydration status was assessed by bioelectrical impedance analysis (BIA), a validated and widely used method that measures biological tissue opposition to the passage of low-intensity alternating electrical current (InBody s10 multi-frequency device, used according to standard manufacturer’ conditions). More specifically, BIA measures resistance (R), i.e., opposition to the flow of electrons (inversely proportional to TBW), and reactance (Xc), i.e., cell membrane opposition to the passage of electrical current (reflecting cell membrane integrity). Using R, Xc, and age, sex, weight, and height data, BIA estimates the following for the whole body and for each of its 5 segments (the arms, legs, and trunk): fat mass, FFM, and muscle mass (in kg and as a percentage of body weight); TBW and TW in each limb (in litres and as a percentage of body or limb weight); ECW and ICW (in litres and as a percentage of TBW); and phase angle (PhA), an indicator of cell membrane functionality, permeability, and integrity. Indicators of whole-body hydration were TBW, TBW/FFM, ICW/TBW (%), ICW/FFM, and PhA, and indicators of right-leg hydration were TW, TW/FFM, ICW/TW (%), ICW/FFM, and PhA. The BIA study was performed in the following conditions: no intense exercise in the previous 24 h, no alcohol consumption in the previous 8 h, strict fasting in the previous 2 h, a toilet visit prior to evaluation, and no evident clinical signs of dehydration.
Muscle function was assessed using the isokinetic test (System 4 Pro device from PRIM), which measures strength (N), work (J), and power (W) in muscle, exercised (throughout the full range of joint movement) at constant speed and maximum tension and fibre activation. Flexion and extension measurements were made at the knee joint. Handgrip strength in the dominant hand was measured using the handheld JAMAR dynamometer. Sarcopenia, established according to the criteria of the European Working Group on Sarcopenia in Older People: 2nd revision (EWGSOP-2), was defined as follows: poor muscle strength according to JAMAR dynamometer-measured grip strength (<27 kg in men and <16 kg in women), and low muscle mass according to the appendicular skeletal mass index (ASM/height2) (<7.0 kg/m2 in men and <5.5 kg/m2 in women according to the BIA). Dynapenia was established as muscle strength below the above-mentioned handgrip cut-off values accompanied by normal muscle mass. Frailty status was established according to the following Fried criteria (19): unintentional weight loss (>5% of initial weight in 12 months), exhaustion (assessed by means of 2 standard questions), low physical activity (no outdoor life or <30 minutes/day outdoor walking), slow walking speed (≥7 s to walk 15 feet), and poor handgrip strength (measured as ≤17 kg in women and ≤30 kg in men using the handheld JAMAR dynamometer). Subjects were classified as robust, pre-frail, or frail for scores of 0, 1–2, ≥3 criteria, respectively. Finally, functional capacity was assessed using the Barthel index, and physical performance was assessed from the TUG test and gait speed.
Statistical AnalysisFor the purpose of sample size estimation, correlations between BIA and isokinetic parameters were the main analyses considered. For an alpha risk of 0.05 and a beta risk of 0.10 in a two-sided test, 113 individuals were necessary to detect a statistically significant correlation coefficient of 0.3.
Continuous variables were described using median and interquartile ranges values, and categorical variables were described using percentages. Normality was tested using the Shapiro–Wilk test. Baseline and 12-month parameters were compared using the Wilcoxon test (paired data). Spearman’s correlation coefficient (rs) was used to assess the relationship between hydration indicators and isokinetic measurement improvements (12-month values minus baseline values). Bivariate linear regression analysis was performed to assess the effect of baseline ICW/FFM on muscle function changes at 12 months, and multivariate linear regression analysis was performed to adjust the effect of baseline ICW/FFM on muscle function changes at 12 months for age, sex, and number of medications. Given that body composition and muscle function differ for men and women, analyses were performed separately by sex. Statistical significance was set to a two sided p < 0.05.
A total of 117 recruited individuals completed baseline BIA and isokinetic testing (mean (SD) age 75.0 (4.1) years, 50.4% women). The main comorbidities were arterial hypertension (62.9%), arthritis (57.8%), dyslipidaemia (49.6%), gastroesophageal reflux disease (19.8%), diabetes (15.5%), peripheral artery disease (15.5%), previous resolved cancer (14.8%), and depression (14.8%). Individuals were taking a mean (SD) of 4.37 (3.02) drugs, 7.0% were considered frail (2 men and 6 women), 3.4% were sarcopenic (2 men and 2 women), and 6.0% had experienced a fall in the previous 3 months. No study participant was using an implanted electronic device.
Assessed at the 12-month follow-up visit were 52 individuals, reflecting a 55.5% loss to follow-up. Reasons for dropping out were voluntary withdrawal (no wish to continue) (62.9%), non-performance of the isokinetic test (due to pain, recent surgery, heart problems, or bone fractures) (18.5%), inability to locate participants (11.1%), and death (3.7%). No age or sex differences were observed between losses and non-losses to follow-up. At follow-up, 3.7% of individuals were considered to be frail (0 men and 2 women) and 7.4 % to be sarcopenic (2 men and 2 women).
Hydration Status and Muscle Function Changes at 12 MonthsTables 1 and 2 report, separately for women and men, 12-month changes in BIA hydration and isokinetic muscle function parameters. TBW decreased by 3.8% in women and by 5.3% in men, PhA decreased by almost 4% in men, and there were no significant changes in ICW%, TBW/FFM, ICW/FFM in neither men nor women. As for muscle function, flexion strength and power decreased in women by 11.8% and 10.0%, respectively, while extension work in men increased by 11.3%.
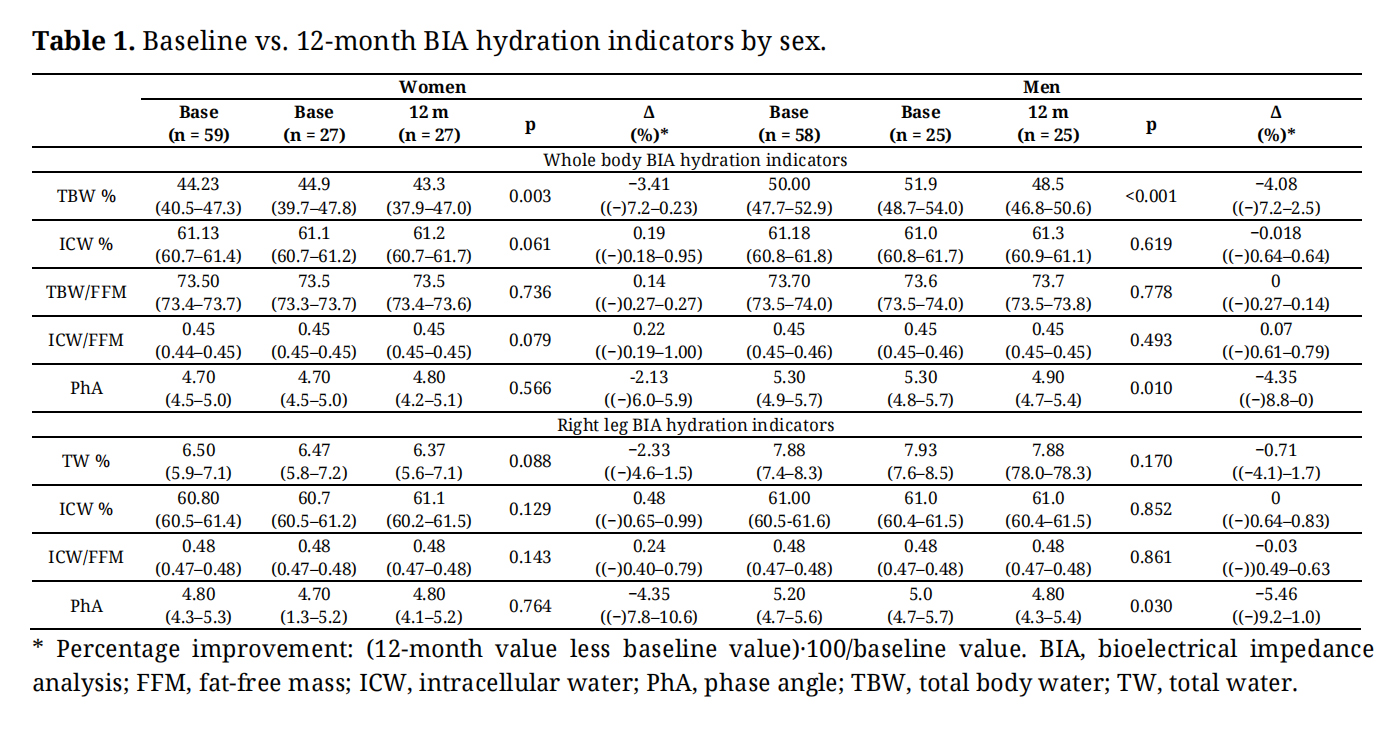 Table 1. Baseline vs. 12-month BIA hydration indicators by sex.
Table 1. Baseline vs. 12-month BIA hydration indicators by sex.
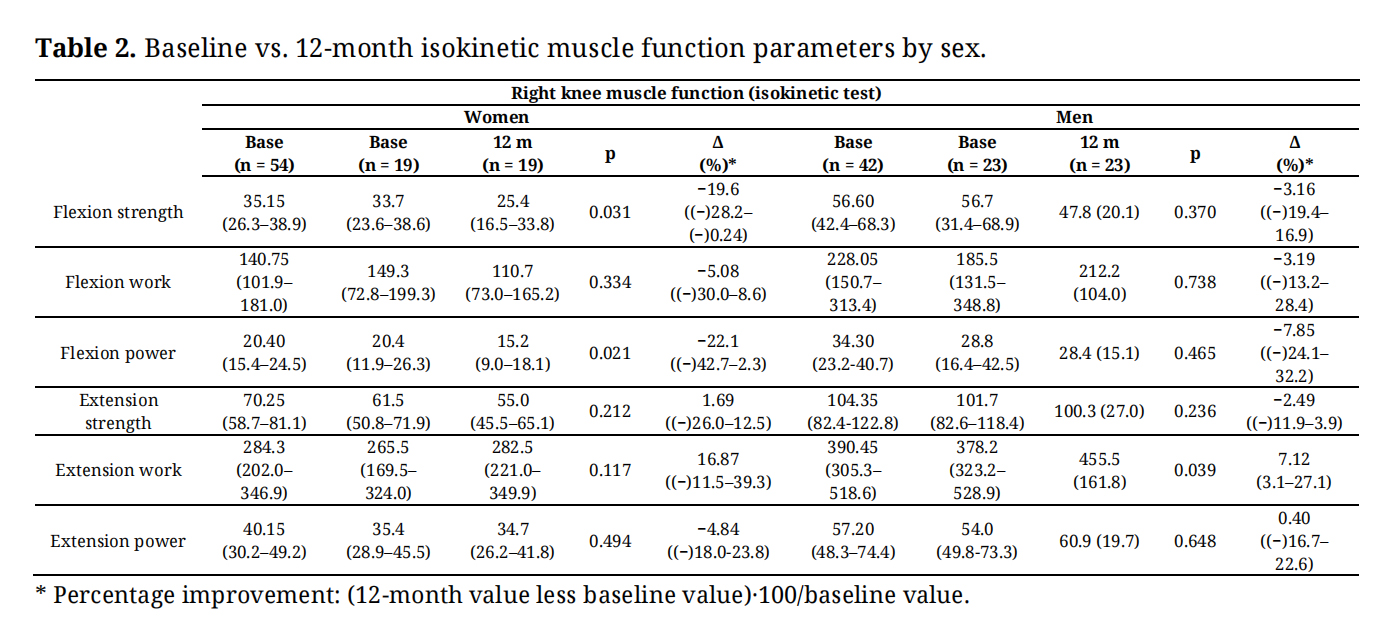 Table 2. Baseline vs. 12-month isokinetic muscle function parameters by sex.
Table 2. Baseline vs. 12-month isokinetic muscle function parameters by sex.
The hydration-muscle function relationship was analysed for both legs, but as no relevant differences were observed between legs, in the interest of brevity we report findings only for the right leg. Table 3 reports, separately for women and men, correlations between baseline right-leg BIA hydration parameters and 12-month improvements in right-leg muscle function. In women, baseline ICW% and ICW/FFM were positively correlated with 12-month increases in extension work (rs = 0.50 [p = 0.028] and rs = 0.47 [p = 0.041], respectively), flexion work (rs = 0.44 [p = 0.058] and rs = 0.41 [p = 0.081], respectively) and flexion power (rs = 0.48 [p = 0.035] and rs = 0.47 [p = 0.042], respectively). In men, baseline ICW% and ICW/FFM were positively correlated with 12-month increases in extension strength (rs = 0.42 [p = 0.053] and rs = 0.44 [p = 0.042], respectively), extension power (rs = 0.46 [p = 0.031] and rs = 0.49 [p = 0.020], respectively), flexion work (rs = 0.41 [p = 0.059] and rs = 0.42 [p = 0.051], respectively), and flexion power (rs = 0.51 [p = 0.015] and rs = 0.53 [p = 0.011], respectively). Baseline PhA was not correlated with an improvement in any muscle function parameter in neither men nor women.
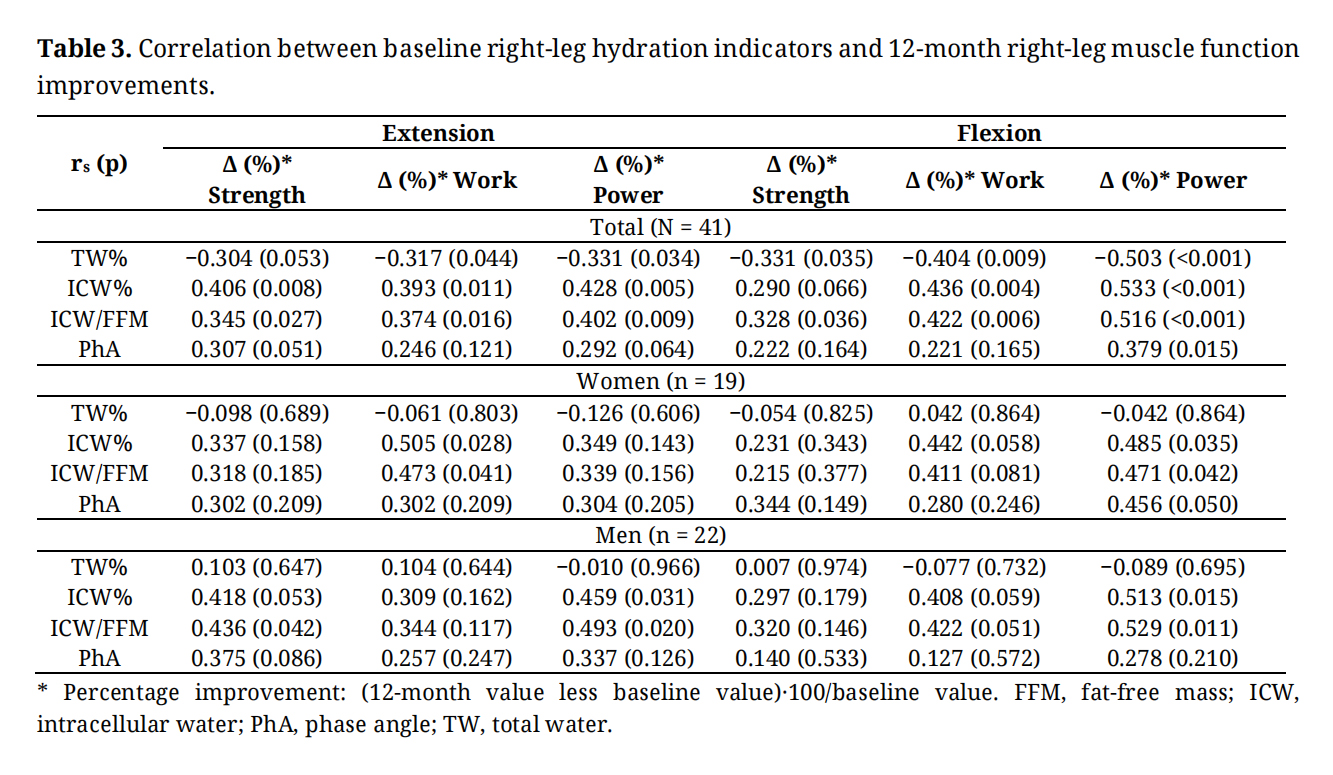 Table 3. Correlation between baseline right-leg hydration indicators and 12-month right-leg muscle function improvements.
Table 3. Correlation between baseline right-leg hydration indicators and 12-month right-leg muscle function improvements.
Finally, Table 4 reports, separately for women and men, the effect of baseline right-leg ICW/FFM on 12-month improvements in right-leg muscle function. After adjusting for age, sex, and number of medications, an independent effect of baseline ICW/FFM was evident for right-leg improvements in extension strength (beta = 1120 N, p = 0.078), extension work (beta = 2356 J, p=0.017), and extension power (beta = 1921 W, p = 0.021), and in flexion strength (beta = 1610 N, p = 0.134), flexion work (beta = 6270 J, p = 0.008), and flexion power (beta = 5183 W, p = 0.003). Figure 1 compares basal and 12-month muscle function parameters by hydration status. Muscle strength and power decreased at 12-month follow-up in subjects with low hydration, while did not change in normo-hydated subjects.
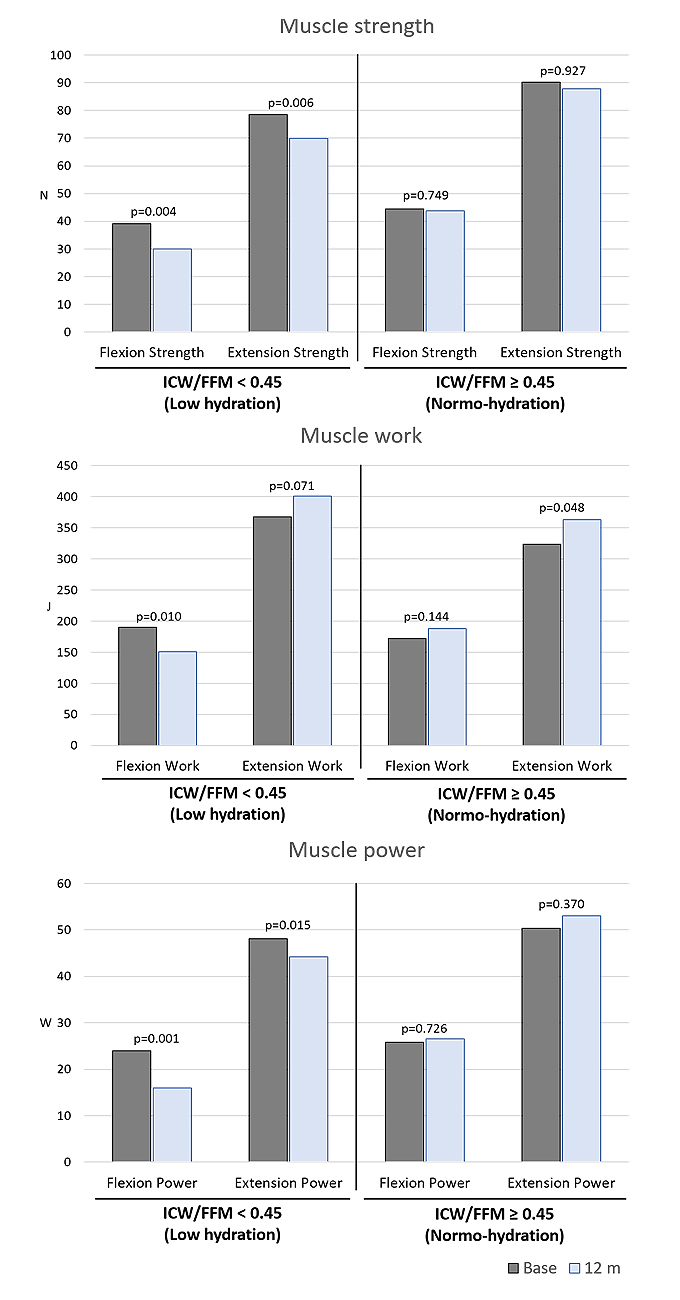 Figure 1. Comparison between basal and 12-month follow-up muscle function parameters by hydration status.
Figure 1. Comparison between basal and 12-month follow-up muscle function parameters by hydration status.
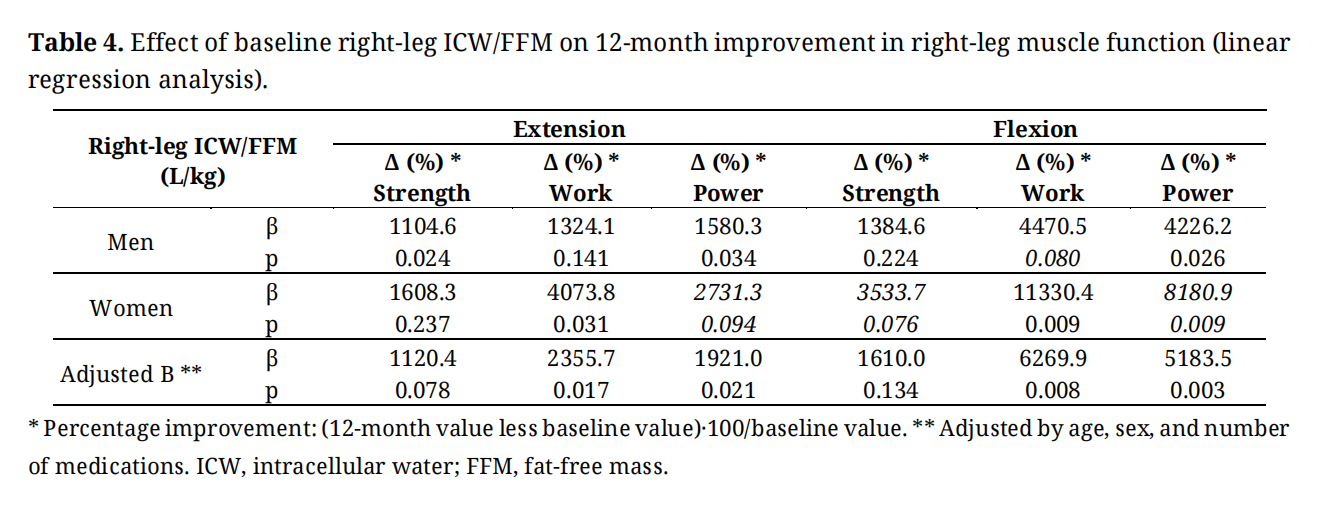 Table 4. Effect of baseline right-leg ICW/FFM on 12-month improvement in right-leg muscle function (linear regression analysis).
Table 4. Effect of baseline right-leg ICW/FFM on 12-month improvement in right-leg muscle function (linear regression analysis).
In men, baseline ICW%, ICW/FFM, and PhA were all correlated with 12-month improvements in gait speed (rs = 0.427 [p = 0.030], rs = 0.467 [p = 0.016], and rs = 0.602 [p = 0.001], respectively), but were not significantly correlated with an improved TUG test or Barthel index. In women, baseline ICW%, ICW/FFM, and PhA were not significantly correlated with 12-month improvements in gait speed, the TUG test, or the Barthel index. Finally, comparing individuals who developed and did not develop sarcopenia during the 12-month follow-up period, baseline ICW% and ICW/FFM were lower in the former (59.2 vs. 61.2 [p = 0.023] and 0.43 vs. 0.45 [p = 0.020], respectively).
For the 12-month study period, our main findings for the population aged ≥70 years were as follows: (a) TBW decreased by approximately 4%, but no significant changes were evident in TBW/FFM, ICW%, or ICW/FFM; (b) in women compared to men, muscle function decline was more pronounced, especially flexion strength and power; (c) independently of age, sex, and number of medications, right-leg baseline ICW/FFM correlated with 12-month increases in knee flexion and extension work and power, while the effect on strength did not reach statistical significance; (d) the lower the baseline ICW%, ICW/FFM, or PhA, the greater the gait speed loss in men; and (e) low baseline ICW/FFM was correlated with a higher sarcopenia risk.
At 12-month follow-up, we observed a 4% reduction in TBW, but no significant changes in ICW or ECW distribution, TBW/FFM, or ICW/FFM. These results point to a water loss proportional to FFM loss, suggesting a reduction in lean mass that was most likely due to reduced muscle mass, but with no clear reduction in hydration status. This interpretation is reinforced by our observation of a 4.5% reduction in lean mass and a 4.7% reduction in muscle mass. However, the fact that we only observed a weight loss of 0.64% indicates a gain in fat mass. Involuntary weight loss—frequent in aged populations and a predictor of increased morbimortality when greater that 4% [17]—is a criterion of the frail phenotype that may be caused by inflammation, comorbidities, medications, poor nutrition, functional limitations, psychological problems, and socioeconomic problems [18]. The ageing process greatly affects skeletal muscle physiology, resulting in muscle mass loss and sarcopenia, and leading to impaired mobility and physical performance [19]. Adequate nutrition and physical exercise may help reduce age-related loss of muscle mass.
We observed that muscle function decreased more in women than men, corroborating scientific evidence of the following: (a) sex hormones play a major role in skeletal muscle homeostasis (testosterone is a potent anabolic stimulus that enhances muscle protein synthesis); (b) age- or disease-related alterations in sex hormones greatly contribute to muscle wasting; and (c) the different hormonal profiles of men and women affect the response to catabolic conditions such as cancer and chronic kidney, liver, heart, and lung diseases [20].
The baseline BIA parameter that best correlated with changes in muscle function, sarcopenia, and physical performance over the 12-month period was ICW/FFM, which is a measure of the amount of ICW per unit of FFM (mostly muscle mass in the lower limbs). Regarding the effect of dehydration on muscle function, our results point to some differences between the sexes. Baseline ICW% and ICW/FFM in women were correlated with 12-month increases in extension work, flexion work, and flexion power, and in men with 12-month increases in extension strength, extension power, flexion work, and flexion power. Although the correlations between baseline hydration indicators and 12-month changes in muscle function parameters did not reach statistical significance in all cases, we are of the opinion that this was very probably due to a lack of sufficient statistical power. Given that the magnitude of the correlation coefficients were similar for both sexes, we speculate that the sex differences could disappear with sufficient statistical power. After adjusting for age, sex, and number of medications, the multivariate linear regression analysis showed a more consistent and robust effect of ICW/FFM on muscle function, with a clear independent effect on muscle work and power and a close-to-significant independent effect on muscle strength. On the other hand, we observed that better hydration (ICW, ICW/FFM) was associated with faster gait speed (although only in men) and a lower sarcopenia risk (both men and women). While the results are not entirely conclusive (partly due to the limited sample size, especially when analysing men and women separately), taken together they indicate a very likely effect of intracellular dehydration on lower-limb muscle function.
Our prospective study results agree with those reported for other cross-sectional studies, thereby broadening the evidence base for the link between hydration status and both muscle strength and physical performance in aged populations [10–13,16]. Leaving aside studies demonstrating that hydration status affects muscle function in young athletes [21], similar results have been reported for aged populations regarding handgrip strength [22] and exhaustion [23,24]. Baseline PhA in our study was not correlated with any muscle function parameter improvements in men or women, and was only correlated with a 12-month improvement in gait speed in men. This finding contradicts Yamada et al. [25], who reported lower PhA in individuals with dynapenia and sarcopenia in their cross-sectional study, and suggested that PhA could be a good indicator of muscle function. Most of our study participants had a quite robust phenotype, with PhA values above the Yamada et al. dynapenia and sarcopenia thresholds. The lack of agreement between that study and ours may be due to differences in mean age (81 vs. 75 years, respectively) and PhA (4.0 vs. 5.3 in men and 3.8 vs. 4.7 in women, respectively), but may be also explained by the poor statistical power of our study.
Our study’s main strengths are its longitudinal and prospective design, the assessment of both hydration and function in the same muscle group (right leg), and use of the isokinetic test, considered the gold standard for assessing muscle function. Study limitations include: (a) the small sample size, which conditioned statistical power, especially in sex subgroup analyses; (b) a high loss-to-follow-up rate related to frailty, which may have diluted the expected 12-month decline in muscle function; (c) a lower than expected prevalence of frailty, suggesting that the study sample was not perfectly representative of a community-dwelling aged population; (d) use of indirect estimates of body water quantity and distribution as measured by BIA, which is not the gold standard for assessing hydration status; and finally, (e) the fact that study participants showed similar hydration levels, with little between-subject variability and no clinically evident dehydration. While the small degree of variability made it difficult to find associations between hydration parameters and muscle function, it nonetheless reflected real-world hydration in an aged population. Further prospective and well-powered studies with participants with a wider range of hydration indicators are required to confirm the hypothesis that dehydration affects muscle function, sarcopenia, and physical performance in aged populations.
In conclusion, BIA indicators of poor lower-limb muscle hydration are correlated with a decline in certain muscle function parameters in the same limb, suggesting that dehydration may affect muscle function in aged individuals. This evidence represents a further step in our understanding of the influence of hydration status on muscle function and physical performance in aged populations. However, better powered studies are necessary to confirm these findings.
The study was performed after approval by the ethics committee of our institution (with reference code: CEIm CSdM 65/19) and that each participant consented to participate in writing before inclusion.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The data that support the findings of this study are not openly available for confidentiality reasons, but are available from the corresponding author upon reasonable request, subject to ethics committee approval.
MSP contributed to the conception and design of the research; IL, JM, PF, EPa contributed to data acquisition and analysis; MC, EB, EPl contributed to data interpretation; and MSP drafted the article. All authors critically revised the article, agree to be fully accountable for the integrity and accuracy of the work, and have read and approved the final article.
The authors declare that they have no conflicts of interest. No AI technologies were used in the writing process.
This study was funded by a grant from the Spanish Ministry of Health-Instituto de Salud Carlos III (ISCIII), reference code PI19/00500, and co-financed by the European Union (FEDER funds).
Internal Family and Community Medicine residents participated in recruiting the study sample.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Serra-Prat M, Lorenzo I, Palomera E, Martínez J, Cuquet M, Burdoy E, et al. Effect of Hydration Status on Lower-Limb Muscle Function in an Aged Population: An Observational Prospective Study. Adv Geriatr Med Res. 2026;8(1):e260003. https://doi.org/10.20900/agmr20260003.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




