Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(2):e250005. https://doi.org/10.20900/agmr20250005
 ,
Jean Woo 1,2,*
,
Jean Woo 1,2,*
1 Jockey Club Institute of Ageing, The Chinese University of Hong Kong, Hong Kong, China
2 Department of Medicine & Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China
* Correspondence: Jean Woo.
Objectives: This review aims to explore the appropriate timing of ACP discussions for individuals with advanced dementia and their surrogates, and the barriers and facilitators of ACP in this population.
Design: A search was conducted on MEDLINE (Ovid), PsycINFO, and CINAHL Ultimate of relevant peer-reviewed research articles up to 13 June 2023. Key words were searched for advance care planning, timing, dementia OR Alzheimer Disease, family surrogate OR member, healthcare worker OR professional, barrier OR facilitator. The authors evaluated the study quality using a pre-agreed checklist of criteria. Relevant article contents were processed via NVivo software to identify the codes, sub-themes, and themes.
Results: 6/42 papers meeting the pre-determined criteria were included from the search. 2 papers identified through other sources were included. A total of 8 papers were included in this review. Primary findings included supportive communication, education interventions, addressing barriers, and utilizing facilitators as important in enhancing the ACP process. The support of healthcare teams to family surrogates in ACP was crucial for improving the quality of dying for individuals with advanced dementia.
Conclusions: Factors affecting the appropriate timing of ACP discussion with people with dementia (PWD) and family include care team taking the initiative to facilitate ACP, early discussions routinely, and updating it periodically. Avoidance, competing priority with current crises and problems, difficulty in accepting future deterioration and challenging to think about death, lacking knowledge on ACP and treatments, feeling as if giving up on PWD in refusing treatment are some ACP barriers. ACP facilitators include PWD and families’ acceptance of the disease trajectory and willingness to address end of life, viewing ACP as support for surrogates for future care decision, education to improve understanding of the disease trajectory, and comfort care to guide decision making, and care team seeing it as a priority.
Advance care planning (ACP) supports adults in understanding and sharing their personal values, goals, and preferences regarding future health care [1]. ACP is a process of communication among a patient with advanced progressive diseases, his/her health care providers, and his/her family members and caregivers regarding the kind of care that will be considered appropriate when the patient becomes mentally incompetent [2].
Patient autonomy is the foundation of ACP [3] which supports patient-centered care, and it is important to facilitate it with the surrogates in person-centered dementia care. In respecting individuals’ autonomy, people are endowed to make healthcare decisions for themselves. PWD has a gradual loss of mental capacity which may compromise the validity of decision for future care. The surrogates play a crucial role in proxy decision-making, particularly if advance discussion is possible. Thus, ACP promotes informed, shared decision-making on goals of care and respects PWD’s autonomy. ACP also provides a relational account of autonomy since the surrogate decision-makers, PWD, and healthcare providers have the opportunity to discuss and gain clarity about the PWD’s care preferences [4].
Discussing ACP for people with advanced dementia (PWAD) is difficult due to the unique disease trajectory. The surrogates may not know their end-of-life (EOL) care preferences. PWAD are prone to have compromised quality of life [5]. It is hypothesized that proper understanding of the people’s ACP may contribute to the quality of their dying and death. By addressing issues facing the surrogates and the healthcare professionals caring for people with advanced dementia, the quality of care for PWAD can be improved.
Dementia is a progressive life limiting illness, and the overall trajectory is characterized by progressive decline [6,7]. There are more severe forms of decline in the later stages of dementia. In addition to the loss of cognitive functions such as memory, thinking, and decision making, an individual with advanced dementia may experience symptoms that affect greater impairment of physical and cognitive functions including severe memory loss and an increased need for help with basic tasks of daily living such as personal care, mobility and eating. There are many barriers that prevent optimal end-of-life care in the final stages of dementia. This deserves our special attention to improve the quality of healthcare for this group of people.
The research questions address the following:
1)
2)
We searched MEDLINE (Ovid), PsycINFO, CINAHL Ultimate for peer-reviewed research articles on ACP with family surrogates of older adults with advanced dementia up to 13 June 2023. Search strategies include key word search for advance care planning, timing, dementia OR Alzheimer Disease, family surrogate OR member, healthcare worker OR professional, barrier OR facilitator. A sample database (MEDLINE) showing the search strategy and its results can be found in Figure 1.
 Figure 1. Database search strategy (MEDLINE Ovid).
Figure 1. Database search strategy (MEDLINE Ovid).
The inclusion/exclusion of the review is defined by the types of population (PWAD) and the stakeholders (surrogates and healthcare professionals), phenomenon of interest (the timing, barriers and facilitators of ACP), the care context of the studies (community, care homes and hospitals), and the types of outcomes (factors on initiation and aspects of consideration for ACP). All primary research, both qualitative and quantitative that reported timing, barriers and facilitators of ACP by the family caregivers, healthcare providers were included. Publication about non-primary research, drug treatment, aging, non-dementia, exploratory studies, pilot studies, case studies, conference paper, early-stage dementia, COVID pandemic related studies were excluded.
Assessment of QualityAuthors evaluated the study quality using a pre-agreed checklist of criteria adapted from a publication [8]. The review protocol for validity assessment is shown in Table 1. Authors evaluated each study individually and discussed it to get consensus.
Each step of the data processing was documented, and records were kept. We abstracted the relevant content from the articles and discussed selected data to get consensus throughout each step of the process. The data were processed via NVivo software to identify the codes, sub-themes, and themes.
This review made reference to Preferred Reporting Items for Systematic Reviews and Meta-Analysis [PRISMA] [9,10]. Title and abstract review were conducted to the relevant articles, and the journal citation report was generated. A PRISMA flowchart was produced as follows (Figure 2).
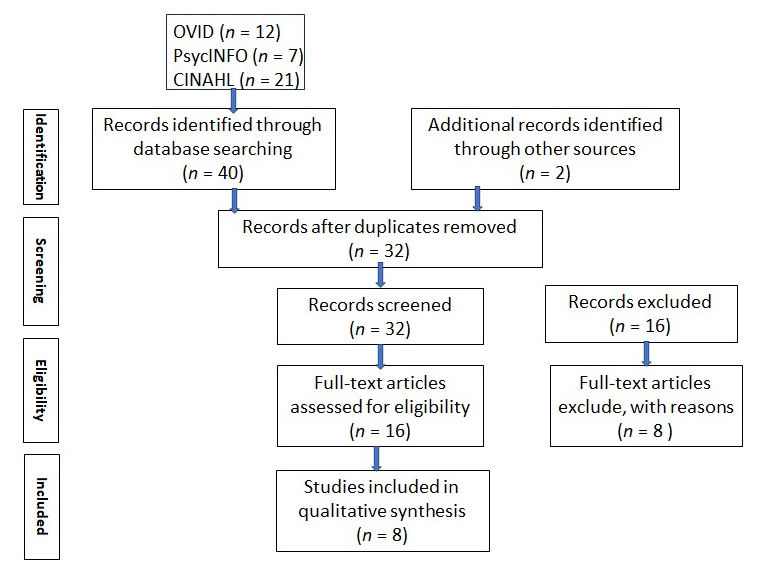 Figure 2. Preferred Reporting Items for Systematic Reviews and Meta-Analysis [PRISMA] flowchart.
Figure 2. Preferred Reporting Items for Systematic Reviews and Meta-Analysis [PRISMA] flowchart.
Critical review of the full articles (n = 16) based on the review protocol for validity assessment from literature [7] is shown in Table 1. Table of validity assessment of the full review articles is tabulated in Table 2. The critical appraisal tools are essential for evaluating the quality and rigor of included studies. Existing and validated tools are instrumental. We used a tool developed by a group of researchers and was adopted for our use for its relevancy in context to our research objectives [8].
 Table 1. The review protocol for validity assessment [8].
Table 1. The review protocol for validity assessment [8].
 Table 2. Table of validity assessment.
Table 2. Table of validity assessment.
We found 40 results from our search, MEDLINE (12), PsycINFO (7), and CINAHL (21). After removal of 10 duplicates, we included 30 papers from our search which met the pre-determined criteria. 16 papers were screened out after reviewing the titles and abstracts. 8 papers were screened out after reviewing the full papers. 2 papers identified through other sources were included. A total of 8 papers were included in this review (Figure 2). Studies of ACP for PWD, particularly exploring the appropriate timing and ACP discussion were scarce. There were unique challenges facing the surrogates of PWAD in the considerations of the appropriate timing, the barriers as well as the facilitators of ACP.
The appropriate time for ACP discussion was uncertain but generally agreed to be early enough for patient participation. When the disease started to become burdensome, ACP was essential. Physicians should initiate it when patients and families were ready to discuss the disease trajectory in a routine encounter. The emotional support in the ACP process was critical.
Lacking knowledge and misunderstanding of treatments and ACP were some common barriers to ACP. Surrogates felt unprepared, ill-informed and confused about EOL care decisions, particularly related to food and hydration. PWD and surrogates avoided the topic, planning, or thinking about deterioration. Their constant dealing with crises and problems were seen as barriers to ACP.
Education intervention improving understanding of disease trajectory and comfort EOL measures, as well as the physicians’ engagement with PWD and their surrogates in ACP conversation were ACP facilitators. Individualized communication, respecting patients’ choice, viewing ACP as support for future care decisions and helping proxies make informed in-the-moment decisions could enhance the ACP process.
Table 3 below summarizes the areas of focus—timing, barriers and facilitators.
 Table 3. Summary of studies regarding the timing, barriers and facilitators of advance care planning.
Table 3. Summary of studies regarding the timing, barriers and facilitators of advance care planning.
It was important to have early end-of-life care discussions when patients were mentally capable but had come to terms with their diagnosis.
ACP Discussion after DiagnosisPatients’ wishes and preferences should be considered, and ACP discussions should be conducted after they have accepted their diagnosis [11]. ACP discussions were found to be most effective between diagnosis and nursing home admission for people with dementia [12]. However, opinions varied on whether ACP should be initiated at the time of diagnosis, with 31% respondents expressing reservations in a survey study [13]. Most respondents believed that the optimal time for initiating ACP should be determined by the patients’ and families’ readiness to face end-of-life issues. They felt that physicians should take the initiative to introduce and encourage ACP. The majority agreed that early discussions would facilitate decision-making during the advanced stages of dementia, as the family would be better prepared.
In the study by Ingavallo et al. [12], both residents and family members believed that ACP should be renegotiated periodically or as needed. According to Sinclair et al. [11], when patients become a burden, it is thought to be a suitable time to initiate the ACP conversation.
Addressing Prognosis on a Routine BasisThe majority (96.2%) of respondents in a survey of general practitioners considered dementia a terminal disease [13]. 37.6% believed that palliative care should apply from the time of diagnosis to severe dementia. Participants opinionated that many family members were unable to accept their loved ones’ prognoses. And not all family carers identified dementia as terminal [6,14], making it difficult to plan ahead for end-of-life care. Uncertainty in the disease trajectory and unexpected events further complicated ACP [15].
Some individuals found ACP discussions confronting, while others appreciated honest conversations about the prognosis to better prepare for the patient’s end of life. Family carers expressed that healthcare professionals were not always honest and open about prognosis leading to emotional shock when informed about a loved one’s impending death [14]. Healthcare professionals could integrate ACP discussions into routine consultations rather than setting aside specific appointments for ACP after individuals had come to terms with the diagnosis [11].
Good Rapport Providing the Foundation for ACPInadequate personal care for nursing home residents and a lack of communication with nursing home physicians were cited as factors contributing to strained relationships and difficulties with ACP engagement [16]. Negative healthcare experiences also posed challenges for ACP discussions [17].
Anxiety of Family Surrogates on Nursing Home AdmissionFamily members expressed elevated levels of anxiety at the time of their loved ones’ nursing home admission and being bombarded with paperwork and end-of-life decisions added to their distress. A direct quote from the family member expressed in the original study [16] best described the internal struggles:
“I just didn’t know what I wanted to do at that point and time. They were bombarding me with paperwork, like sign this and sign that and then they asked me to make end-of-life decisions and that is the last thing that you want to do as you put your loved one in the nursing home”.
It was commented that organizational requirements might necessitate completing paperwork and discussing end-of-life decisions. Sensitivity and allowing families more time to process information could help alleviate their stress. Yet, at the practical level, it was important to have these discussions early to prevent future distress in the event of unplanned hospital admissions [15].
Competing PrioritiesFamily members often did not realize the urgency of ACP until it was too late, and the person with dementia had lost the capacity to have the discussion. Constantly dealing with crises and immediate problems could lead to ACP being perceived as a lower priority for patients, caregivers, and healthcare professionals [11]. Supporting proxies in making decisions was crucial, as ambivalence towards ACP was more pronounced in people with dementia. Uncertainty about the appropriate timing of ACP discussions aroused from the emotional challenges of reflecting on deterioration at the end of life compared to planning for death itself. Thinking about deterioration appeared more challenging than thinking about death. While some PWD were ready to engage in EOL care discussions, most preferred focusing on the present and rationalizing that their families did not require direction for future care.
The identified barriers to ACP included the fear of provoking anxiety, lack of understanding of EOL care options and the treatment limitations, and lacking support from the healthcare team. They were categorized into those related to the healthcare team, and those related to the patients and family members.
Barriers Related to the Healthcare TeamVarious sentiments towards ACP from the healthcare team impeded the progression of ACP with patients and family proxies. End-of-life conversations were recognized as emotionally sensitive and had implications for professional and legal responsibilities, which could make healthcare professionals hesitant to initiate ACP discussions [15]. Some healthcare professionals also preferred to postpone ACP discussions to avoid confronting mortality and causing distress to patients and themselves [13]. Additionally, Clinical Commissioning Groups were uncertain regarding the necessity of specific dementia palliative care services, which could impact the availability and prioritization of ACP [14].
The uncertainty surrounding the disease trajectory and unexpected events further complicated ACP discussion. Healthcare professionals struggled to determine the appropriate timing to initiate ACP due to this uncertainty [12]. This could lead to a perception that healthcare professionals were not being honest and open about the prognosis with family proxies [14]. Poor relationships with care staff at nursing homes, inadequate communication, and suboptimal resident personal care could also hinder ACP discussion [16]. Additionally, the constant dealing with crises and immediate problems might lead to ACP being perceived as a lower priority by patients, caregivers, and healthcare professionals [11].
Barriers Related to Patients and Family SurrogatesBarriers related to the patients and family members included the fear of unnecessarily increasing anxiety among patients and family during end-of-life care discussions [13]. Family members might have difficulty accepting the prognosis of PWD and struggled to understand treatment options and the limitations of life-sustaining treatments [12,13]. This could result in uncertainty and confusion regarding end-of-life care decisions, particularly related to food and eating, and avoidance of discussions about end-of-life care [14].
For patients with dementia, ACP discussions could be frightening, and they might prefer to focus on the present rather than thinking about deterioration or death [12,17]. Negative healthcare experiences could create barriers to engaging in ACP. Some residents were more interested in informal planning rather than formal advance directives [17]. There could also be distrust toward the appointment of a proxy, living wills, and uncertainty about the legal status of ACP and advance directives [12]. Some individuals had difficulty finding the “right” proxy and worried about others taking advantage of their role as proxies. It was common for residents to report that their children were unwilling to discuss ACP [12,14]. Moreover, PWD who lack close family or friends might require more support from service providers to engage in ACP [17].
Family caregivers are often left unprepared and ill-informed about ACP, with limited knowledge and little involvement in structured ACP discussions [12,14,17]. Other barriers included stress at the time of nursing home admission, lack of communication with nursing home physicians, exclusion from medical decisions, difficult end-of-life decisions such as the use of feeding tubes, and insufficient information to guide surrogate decision-making [12,16].
The facilitators can be categorized into those related to the healthcare team and those related to the patients and family members.
ACP Facilitators of the Healthcare TeamThe healthcare team played a crucial role in facilitating ACP discussions and decision-making. Some of the facilitating factors included emotional, education and guidance, communication and collaboration and palliative care specialists.
Providing emotional support to families upon admission of the patient could create a supportive environment for ACP discussions [16]. This support could help alleviate anxiety and create a safe space for discussions. Healthcare professionals could educate families about the prognosis of dementia and provide information on treatment options and common decisions, such as the treatment of feeding problems [16]. By providing clear explanations and guidance, healthcare professionals could empower families to make informed decisions. Improved communication and collaboration between healthcare professionals and families could facilitate the ACP process [16]. Sharing information and maintaining enduring working relationships, especially with palliative care specialists, helped support and validate the decisions made during ACP [15]. The involvement of palliative care specialists was instrumental in facilitating ACP discussions and decision-making [15]. Their expertise and presence in care homes provided guidance and support for the healthcare team and contributed to the continuity of care.
ACP Facilitators of the Patients and Family MembersPatients and family members played a crucial role in the ACP process. Some of the facilitating factors included willingness to engage, external facilitators, family support and enhanced rapport.
Residents with dementia and their family members were willing to engage in ACP discussions [12]. Residents saw ACP as an opportunity to express their opinions, while family members valued the usefulness of ACP in planning for the future. The involvement of external facilitators to the family, such as trained ACP facilitators, healthcare professionals or care home staff, could help initiate and catalyze ACP conservations [12]. These facilitators could provide guidance, support, and education to residents and their families, enhancing the ACP process [18]. ACP was seen as a mechanism for PWD to support their families [17]. The idea that engaging in ACP could alleviate future burdens for family members was a motivating factor for PWD. Building a solid rapport between care home staff and family caregivers facilitated the ACP process [14]. Care home staff with greater experience in end-of-life dementia care could instill confidence and trust in family caregivers, creating a supportive environment for ACP.
Despite decision-making not being a term particularly searched for; the theme decision-making kept emerging in data synthesis. It could be an important concept behind the ACP process regarding timing, barriers and facilitators. Factors influencing the decision making in ACP were also noted. A summary of the major themes—timing, barriers and facilitators of ACP as well as decision making are tabulated in Table 4 below:
 Table 4. Summary of the identified major themes.
Table 4. Summary of the identified major themes.
Knowledge gained from this review can be useful to inform healthcare professionals on how to enhance the ACP process to improve care for patients with advanced dementia and their families.
Timing of ACPDetermining the appropriate timing for ACP initiation can be challenging and should be individualized. Factors such as the patients’ and families’ willingness to face the diagnosis and prognosis of dementia, as well as their readiness to engage in end-of-life discussions, should be considered. ACP discussions can be introduced on admission to a nursing home by providing information and educational materials to prepare families for follow-up discussions. Regular reviews and periodic ACP discussions can be beneficial. Healthcare professionals should take the initiative to introduce and encourage ACP, while addressing the educational needs of families in caring for PWD. Patients and proxies may like to focus on the here and now than planning for end-of-life care as they are constantly challenged by the crises and current problems triggered by advanced dementia. Physicians or the healthcare team should take the initiative to introduce and encourage ACP as well as address the need for improved knowledge to involve families in caring for PWD. Early discussions would facilitate decision-making during the more advanced stages of dementia, as the family would be better prepared. The appropriate time is cited as between diagnosis and nursing home admission and with periodic review. ACP is more receptive when conducted on a routine basis with good support for education and the emotional needs of the proxies from the healthcare team.
Decision-MakingMany patients with advanced dementia and family surrogates have limited knowledge of ACP. They often feel that they are unprepared and do not know where to get help in making clinical decisions. They struggle with decision-making due to a lack of understanding of the limitations and complications of life sustaining treatments, especially tough decisions relating to hydration and nutrition. Some residents prefer an informal sharing of ACP to officially appointing a proxy or signing of documents. Residents’ life stories can be used to inform ACP and communicate a shared understanding to care home staff of what should be prioritized. ACP is also a way for PWD to support their families. More direct conversation could help proxy make more informed in-the-moment decisions.
Education and support interventions can help address these challenges and improve decision-making. Shared decision-making between healthcare professionals, patients, and proxies should be prioritized, with respect for the patients’ choices and individualized communication. It is important to involve PWD early in decision-making and consider their wishes and preferences before they have lost their mental capacity to participate. Emotional support should be provided to proxies, and research evidence should be shared to alleviate their internal struggles and concerns. Clear roles and responsibilities should be established in care homes to facilitate discussions and decision-making, and a better understanding of the effects of advanced dementia can enhance planning in end-of-life care.
ACP BarriersAdvance care planning is crucial for supporting PWD in planning future care that aligns with their values and preferences. However, there are significant barriers that need to be addressed to facilitate the ACP process.
Patients and families face barriers such as lack of knowledge about ACP, difficulty accepting the diagnosis and prognosis, and challenges in understanding the limitations of life-sustaining treatments. They may also have concerns about appointing proxies, stress or emotional overload, low education levels, or mental incapacity. Other barriers include participating too late, difficulty identifying appropriate proxies, and unawareness that ACP can be altered.
Healthcare professional related barriers include emotionally sensitive conversations, implications for legal responsibilities, uncertainty in disease trajectory, and avoidance of discussion prognosis due to fear of distressing the patient or themselves. There is also uncertainty about the necessity of dementia palliative care, as well as time constraints and assumptions that ACP is not a priority for patients.
ACP FacilitatorsThe identified ACP facilitating factors providing emotional support to families upon admission, educating them about the prognosis to guide decision making, improving resident care, and enhancing communication with healthcare professionals. Separating ACP from the immediate admission process, educating family members about dementia, explaining treatment options, and establishing therapeutic relationships can also be beneficial to ACP discussions. Care home routines and policies play a role in determining responsibilities and decision-making processes. External facilitators can act as catalysts for ACP conversations, and ACP can be framed as an act of care that supports families. Continuity of care and knowing the wishes of PWD are essential, and care home staff with experience in end-of-life dementia care can provide valuable support. Well-defined outcomes of good end-of-life care and developing relationships with family carers are also important goals.
Studies were mainly conducted with convenient samples. Biases may be present, such as participants who had extreme experiences and were motivated to share. The included studies were mainly from the nursing home setting, so caution should be taken when applying them to other settings. The selection of quality appraisal tools as well as the evaluation based on the tools may involve some subjective elements which may contribute to biases in the results and conclusions. Heterogeneity of the studies may yield different outcomes potentially contributing to biases.
Factors affecting the appropriate timing of ACP discussion with PWD and family include physicians taking the initiative to introduce and encourage ACP, early discussions once PWD and families accepting the diagnosis and prognosis, and touching on ACP routinely, and renegotiating it periodically. Avoidance, denying the need to plan, not a priority for constant dealing with crises and problems, difficulty in accepting future deterioration and challenging to think about death, lacking knowledge on ACP and the life-sustaining treatments, feeling as if giving up on PWD in refusing treatment are some ACP barriers. ACP facilitators include patients and families’ acceptance of the disease trajectory and willingness to address end of life, viewing ACP as support in patient’s future care decision, education to improve understanding of the disease trajectory, and comfort care to guide decision making, physicians taking the initiative to introduce and encourage ACP, and to explain the consequences of medical decisions.
Ethical approval is not applicable, because this review article does not contain any studies with human or animal subjects.
The review was registered with PROSPERO ID: CRD42023442617 on 19 July 2023.
All data generated from the study are available in the manuscript. The data is available from the Chinese University of Hong Kong (CUHK) as a part of PhD thesis on completion.
Conceptualization, FC and JW; Methodology, FC; Software, FC; Validation, FC and JW; Formal Analysis, FC; Investigation, FC; Resources, FC; Data Curation, FC; Writing—Original Draft Preparation, FC; Writing—Review & Editing, JW; Visualization, FC; Supervision, JW; Project Administration, FC; Funding Acquisition, JW.
The authors declare that they have no conflicts of interest.
The study was supported by the Hong Kong Jockey Club as part of the end-of-life care capacity-building education program.
The authors wish to thank Kendy Lau, Associate Medical Librarian, CUHK for her advice in the literature search.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Chan F, Woo J. Factors Affecting the Initiation and Consideration of Advance Care Planning (ACP) with Surrogates of Older Adults with Advanced Dementia: A Systematic Review. Adv Geriatr Med Res. 2025;7(2):e250005. https://doi.org/10.20900/agmr20250005

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




