Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(2):e250006. https://doi.org/10.20900/agmr20250006
 ,
Abigail Anderson 2 ,
Laurie Neely 2,* ,
Christina Speranza 2 ,
Caitlyn Wilkerson 2 ,
Jennifer Tolle 2 ,
Kathleen Salik 3 ,
Rolando Lazaro 4 ,
Morris Casano Beato 2
,
Abigail Anderson 2 ,
Laurie Neely 2,* ,
Christina Speranza 2 ,
Caitlyn Wilkerson 2 ,
Jennifer Tolle 2 ,
Kathleen Salik 3 ,
Rolando Lazaro 4 ,
Morris Casano Beato 2
1 Select Physical Therapy, 501 East Oak Street, Suite D, Kissimmee, FL 34744, USA
2 Doctor of Physical Therapy Program, Division of Physical Therapy, School of Kinesiology & Rehabilitation Sciences, University of Central Florida, 12805 Pegasus Drive, HS-1 Room 256, Orlando, FL 32816, USA
3 Banner Physical Therapy in Partnership with Select Medical, 5605 Eugie Avenue, suite 215, Glendale, AZ 85304, USA
4 Department of Physical Therapy, College of Health and Human Services, California State University, 6000 J Street, Sacramento, CA 95819, USA
* Correspondence: Laurie Neely.
Background and Introduction: As the prevalence of Parkinson’s disease (PD) increases, novel treatment methods are sought to slow the disease progression. Because medication loses effectiveness with prolonged use, deep brain stimulation (DBS) can become a surgical option. There are positive outcomes with the use of amplitude-based training (ABT) as treatment for persons with PD (PwPD), but little research has been done to support its effectiveness for individuals with DBS.
Purpose: The purpose of this retrospective case series is to investigate the effects of ABT on people with and without DBS. We hypothesize that ABT will produce improvements on mobility outcomes in PwPD regardless of DBS status.
Methods: Data was collected from 7 PwPD with DBS, forming the DBS+ABT group. Seven PwPD without DBS were matched based on age, gender, and ambulation status, forming the ABT group. All 14 participants received ABT following the Lee Silverman Voice Therapy BIG protocol for 16 weeks. Outcome scores to assess functional leg strength, mobility, and balance were measured pre and post intervention. A repeated measures ANOVA was performed with pre to post as the within group factor and group assignment as the between group factor.
Results: No significant interaction effects were found. Significant main effects of time were found for mobility and strength outcomes. Both groups improved from pre to post, but groups did not differ.
Conclusions: The findings of this study indicate that ABT may be an effective intervention to improve functional leg strength, mobility, and balance for both PwPD with and without DBS.
PD, Parkinson’s disease; PwPD, persons with Parkinson’s disease; ABC, Activities-specific Balance Confidence Scale; ABC-6, Short Version Activities-specific Balance Confidence Scale; FTSTS, Five Times Sit to Stand; TUG, Timed Up & Go; DBS, deep brain stimulation; ABT, amplitude-based training; ANOVA, analysis of variance; LSVT, Lee Silverman Voice Therapy
Idiopathic Parkinson’s Disease (PD) is a progressive neurodegenerative disorder that affects the dopamine system of the basal ganglia. The exact etiology of the disease is unknown, but there is an association with male gender, older age, and family history [1,2]. PD is the second most common neurodegenerative disease behind Alzheimer's disease with a prevalence of nearly one million people diagnosed in the United States and seven million individuals worldwide. The prevalence is estimated to double by 2040 [3,4].
PD is a slowly progressing disease, as symptoms only begin to occur after 30%–60% of degeneration has already occurred. The main neuropathological findings in persons with PD (PwPD) consist of degeneration of dopaminergic neurons and the development of Lewy bodies which result in varying motor and non-motor symptoms [5–7]. Motor symptoms pertain to having difficulty with linking the intent to move with actual movement, resulting in bradykinesia, rigidity, and postural instability. PD is also closely associated with a resting tremor, freezing, and shuffling gait. Non-motor impairments include depression, cognitive dysfunction, sleep disorders, and autonomic dysfunction. Individuals with PD are classified using the Hoehn & Yahr scale (H&Y), consisting of five stages that are based on the degree of motor impairment.
Atypical parkinsonism refers to progressive neurological diseases that have the same or similar symptoms as PD but have differing etiologies and therefore do not respond well to typical Parkinson’s treatments. Some of the most common types of atypical parkinsonism include Multiple Systems Atrophy, Lewy Body dementia, progressive supranuclear palsy, and corticobasal degeneration [8].
The current gold standard treatment for PD is a combination of pharmacologic, surgical, and physical/occupational/speech therapy treatments [9]. First-line pharmacologic treatment usually involves levodopa, a dopamine replacement agent, to address symptoms relating to dopamine deficiency. Some of the side effects of levodopa may increase risk of falls including dizziness, weakness, confusion, and alterations in sensation [10]. Long-term levodopa use can result in “wearing off” effects; therefore, dopamine agonists, carbidopa, or MAO-B inhibitors may also be used [9].
Physical and occupational therapy interventions are also often used as an adjunct to medication and/or surgical intervention to help slow the progression of the disease and reduce cognitive and motor impairments. Utilizing this interdisciplinary strategy for treatment has proven to be the most cost-effective approach across the lifespan [9]. These therapies often work on achieving bigger movements of the trunk and extremities that translate to gait and anticipatory and reactive balance to improve mobility and reduce risk of falls. There is currently a lack of research on the utility of specific physical therapy interventions, with most research vaguely listing strength training, balance training, aerobic exercise, and treadmill training as the modalities used [11].
Lee Silverman Voice Treatment (LSVT) is an approach that was originally developed to address the vocal changes and dysarthria that often develops during the course of PD, and was termed LSVT-LOUD treatment [12]. Current literature exists determining the effectiveness of LSVT-LOUD for addressing these problems in the PD population [13,14]. More recently, another segment of LSVT that focuses on amplitude based training (ABT) termed LSVT-BIG, was developed to address the motor deficits in the trunk and limbs associated with PD [12]. Individuals with PD often demonstrate slow and small amplitude movements. To address these deficits, a physical or occupational therapist can use ABT which focuses on whole body movements to improve speed and amplitude of daily functional tasks [12]. The four week long ABT protocol is often integrated into traditional physical or occupational therapy care by LSVT certified therapists. There is moderate evidence available to support the effectiveness of ABT for improving motor function in individuals with PD without DBS [12]. This treatment approach is thought to work by promoting larger-amplitude movements to overcome Parkinson-associated hypokinesia and modify the person’s perception of their movements [12].
A common surgical strategy for treating more advanced PD is deep brain stimulation (DBS). DBS involves implanting a device into either the subthalamic nucleus or globus pallidus internus that emits electrical impulses to correct motor changes secondary to the disease process [9]. DBS helps reduce the amount of medication the patient requires across the lifespan, with the tradeoff of potentially having remaining mild motor symptoms [9]. DBS is currently not recommended for treating atypical parkinsonism as it can be associated with increased cognitive impairments and there is not yet enough existing literature to support its safety in this population [15]. At this time, there is a gap in the literature on the effectiveness of ABT versus traditional physical therapy for treating PwPD that have also undergone DBS.
The purpose of this study is to investigate the effects of ABT on PwPD with DBS and PwPD without DBS. We hypothesize that there is no difference between the two groups with respect to changes in scores in the outcome measures for balance confidence, functional lower extremity strength, and general mobility. Since it has been shown in the literature that ABT improves motor and functional mobility in PwPD we hypothesize that ABT interventions will likely produce similar benefits to PwPD with or without DBS.
A retrospective analysis was conducted using electronic patient records from 2 outpatient physical therapy clinics, one in Arizona and one in Florida, after review by the University of Central Florida Institutional Review Board to protect the rights and welfare of human participants on April 6, 2020. The outpatient clinics granted access to the patient records that met the inclusion criteria to 2 members of the research team who independently extracted the data variables of interest and then transferred the de-identified information to the other researchers for analyses.
A master list was obtained from the outpatient clinics of PwPD referred to physical therapy during the designated timeframe. From the master list of PwPD, charts were selected for inclusion in the study if an individual had been referred to outpatient physical therapy to address decline in motor symptoms and functional mobility from April 2016 and February 2022, at the time of referral the person has diagnosis of PD, and the individual had received amplitude-based training intervention. Exclusion criteria included any medical comorbidities that hindered an individual from participating in ABT intervention, being bed-bound or chair-bound (Hoehn & Yahr stage 5), or having a level of cognitive impairment where they were unable to follow the ABT protocol. Two groups of PwPD were created. First, seven PwPD who received DBS were identified (DBS+ABT). Thirty-nine additional patients without DBS that completed ABT were examined to determine the age, sex, and ambulation matched controls. Seven PwPD who were matched with the first group based on age, gender, and ambulation status were identified and selected for the second group (ABT).
Data ExtractionA paper and computer-based extraction spreadsheet was utilized to collect participant demographics in addition to preintervention and post-intervention scores for the Activities-specific Balance Confidence (ABC) Scale, Five Times Sit to Stand Test (FTSST), and Timed Up & Go (TUG). A computer-based extraction form was tested using a medical record that was excluded from the analyzed sample. There was a total of 14 charts that were included in this study.
Outcome MeasuresThe primary outcome measures utilized in this study include the ABC-6 Scale, FTSST, and TUG. The individuals were assessed using the outcome measures on the day of their initial evaluation (baseline) and on the day of their final physical therapy session (discharge) to determine any progress following the ABT intervention.
The ABC scale is a 16-item self-report measure that assesses an individual’s percentage level of confidence in various daily activities including walking around the house, sweeping the floor, walking in a crowded mall, and walking on slippery floors [16]. The overall score is an average of the percentage confidence for each measure (0 = no confidence; 100 = complete confidence). A cut-off score of <69% was found to be predictive of recurrent falls in the next 12 months [17]. This measure is recommended for PwPD of H&Y stages 1–3 by the Parkinson Evidence Database to Guide Effectiveness (PDEDGE) [18]. A short version of the scale, ABC-6 Scale which includes the 6 most challenging items, was developed for efficient use in the clinical setting. The ABC-6 Scale has been found to be as valid as the complete ABC scale [19]. A cut-off score of ≤60% has been determined to distinguish between fallers and non-fallers for the ABC-6 Scale [20].
The FTSTS is a measure of functional lower extremity strength demonstrated by having the participant stand up from a seated to a fully standing position five times as fast as they are able to perform without the use of the upper extremities. A cut-off score of more than 16 seconds has been established to demonstrate increased fall risk in persons with PD [21]. This measure is highly recommended for PwPD of H&Y stages 1–4 by the PDEDGE [18].
The Timed Up & Go test is an assessment of mobility. In this measure, the time it takes a participant to stand from a chair, walk three meters, turn around, and walk back, and sit down on the chair is recorded. A cut-off score of 11.5 seconds has been established to demonstrate increased fall risk in PwPD [22]. The TUG is highly recommended for PwPD of H&Y stages 1–3 by the PDEDGE [18].
Amplitude-Based Training ProcedureAll participants from both groups received similar ABT and ABT-based functional mobility training as their physical therapy intervention. In consultation with the patients, the shared decision was made to implement this type of intervention to address these impairments of hypokinesia and rigidity. The ABT certified clinicians administered the intervention in 1:1 manner with an ABT protocol of 60-minute sessions, for four sessions per week, for four weeks for a total of 16 sessions. The ABT protocol consists of eight exercises that are traditionally completed for one set of ten repetitions including: seated floor-to-ceiling reaching, seated side-to-side reaching, forward stepping, lateral stepping, backward stepping, forward rock-and-reach, sideways rock-and-reach, and sit-to-stands [23]. Standing exercises can be modified to sitting exercises if the individual is in later stages of PD with more severe motor deficits and/or has better postural stability in a seated position. The seated versions of the exercises also emphasize large movements at the lower extremities and upper extremities. The exercise program included amplitude-based functional task training such as sit to stands, dressing activities, and bed mobility activities. Interventions included education on community exercise plans including cycle ergometry and recumbent stepping, reiterating the movements performed in the ABT protocol.
Deep Brain StimulationThe DBS+ABT group had previously received DBS. Six out of seven patients in the DBS+ABT group had bilateral DBS while one individual had right-sided DBS. Timing of DBS ranged from one to nine years prior to initial outcome scores being collected and the initiation of ABT.
Timing of MedicationParticipants in the ABT group received therapy sessions while in the “on” phase of the dopaminergic medication to facilitate motor function and movement. The DBS group medication was not tracked as participants reported improved motor function post-DBS and most report stopping the use of dopaminergic medications post-DBS. After DBS surgery and the initial programming phase of the brain stimulation is completed, a stabilization period from 3–6 months post-operation allows for weaning of dopaminergic medications [24].
Data AnalysesStatistical analysis was performed with IBM SPSS Version 29 (Armonk, NY, USA). An independent t-test was used to compare the pre and post intervention difference in the outcome measures between the 2 groups. Descriptive statistics were obtained for the total sample and by group. An alpha level of p < 0.05 was used for determining significance.
Data were extracted from 14 medical records by hand-searching using the computer and paper-based data extraction tool. The total mean age of the participants was 63.92 (SD = 8.53) years, 100% were male and the median H&Y stage is 2. The total mean age of the DBS+ABT group was 64 (SD = 8.16) years, and the median H&Y stage is 3. The total mean age of the ABT group was 63.85 (SD = 9.54) years, and the median H&Y stage is 2. Approximately 28.57% (n = 2) of the DBS +ABT group uses an assistive device while 14.28% (n = 1) of the ABT group use an assistive device for ambulation. Table 1 summarizes the demographic information of all patients. There were no significant differences between groups in the primary outcomes of balance confidence, functional lower extremity strength, and general mobility.
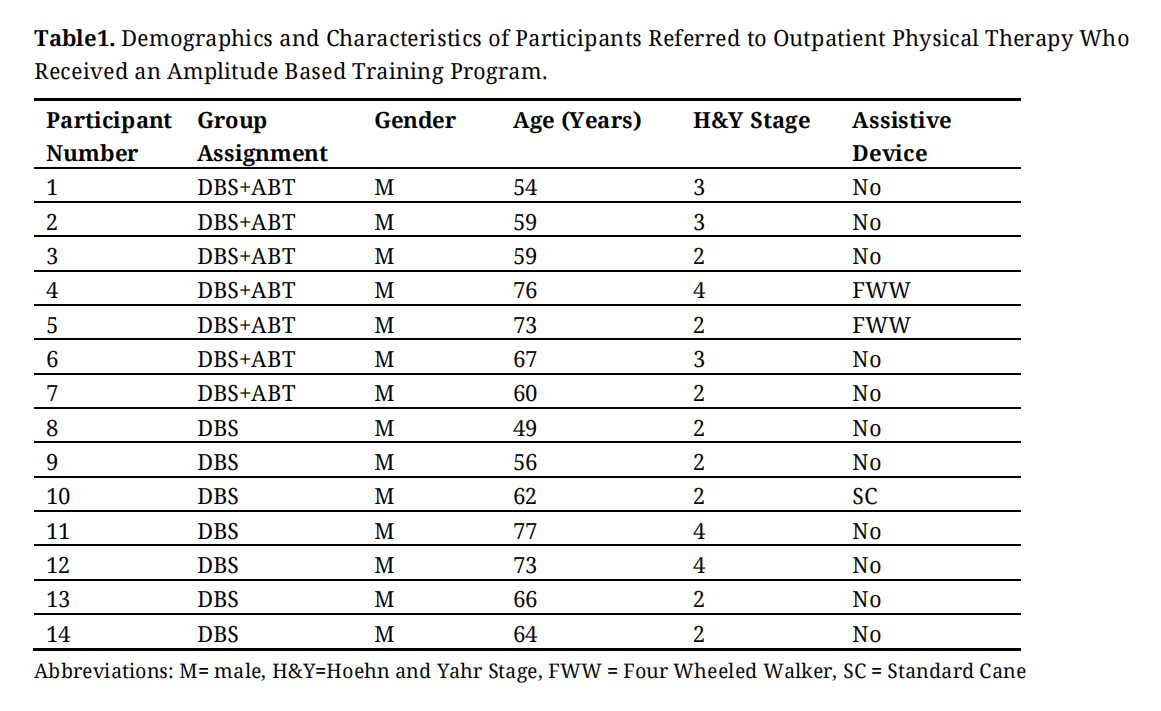 Table 1. Demographics and Characteristics of Participants Referred to Outpatient Physical Therapy Who Received an Amplitude Based Training Program.
Table 1. Demographics and Characteristics of Participants Referred to Outpatient Physical Therapy Who Received an Amplitude Based Training Program.
The results of the descriptive statistics showed that the DBS+ABT group had lower values for the ABC-6Scale percentage score difference before and after intervention (M = 14.8, SD = 19.36) than the ABT group (M = 15.93, SD = 16.56). The results of the descriptive statistics also showed that the post interventions ABC-6 Scale percentage scores for the DBS+ABT group (M = 60.65, SD = 20.32) and the ABT group (M = 59.93, SD = 23.53) were at the cut off score of 60% that distinguishes between fallers and non-fallers secondary to balance confidence (Figure 1) [20].
The Levene test of equality of variance yielded a p-value of 0.721, which is above the 5% significance level. The Levene test was therefore not significant and the null hypothesis that all variances of the groups are equal was not rejected. Thus, there was variance equality in the samples.
A two tailed t-test for independent samples (equal variances assumed) showed that the difference between the two groups with respect to the ABC Scale percentage score difference before and after intervention was not statistically significant, t(10) = −0.11, p = 0.918, 95% confidence interval [−24.99, 22.73]. Thus, the null hypothesis was not rejected.
The effect size d was 0.06 (equal variances assumed). With d = 0.06 there was a very small effect [25].
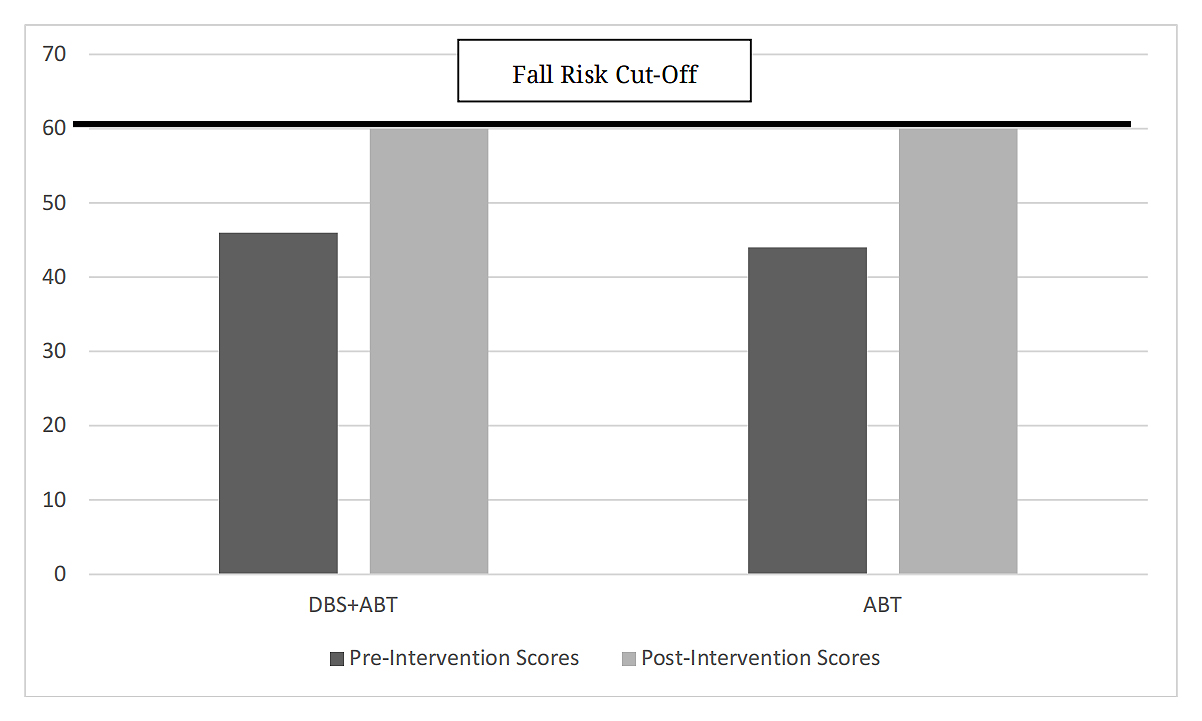 Figure 1. Activities-specific Balance Confidence—6 Scale score before and after Amplitude Based Training intervention.
Figure 1. Activities-specific Balance Confidence—6 Scale score before and after Amplitude Based Training intervention.
The results of the descriptive statistics showed that the DBS group had higher values for the FTSTS time difference before and after intervention (M = 3.12, SD = 4.43) than the ABT group (M = 1.71, SD = 4.54). The results of the descriptive statistics also showed that the post interventions FTSST time for the DBS+ABT group (M = 12.33, SD = 2.71) and the ABT group (M = 13.5, SD = 7.56) make the cut off score of 16.0 seconds to be classified as no longer a fall risk based on the lower extremity strength after the ABT intervention (Figure 2) [21].
The Levene test of equality of variance yielded a p-value of 0.621, which is above the 5% significance level. The Levene test was therefore not significant and the null hypothesis that all variances of the groups are equal was not rejected. Thus, there was variance equality in the samples.
A two tailed t-test for independent samples (equal variances assumed) showed that the difference between the two groups with respect to the FTSTS time difference before and after intervention was not statistically significant, t(11) = 0.56, p = 0.585, 95% confidence interval [−4.09, 6.9]. Thus, the null hypothesis was not rejected.
The effect size d was 0.31 (equal variances assumed). With d = 0.31 there was a small effect [25].
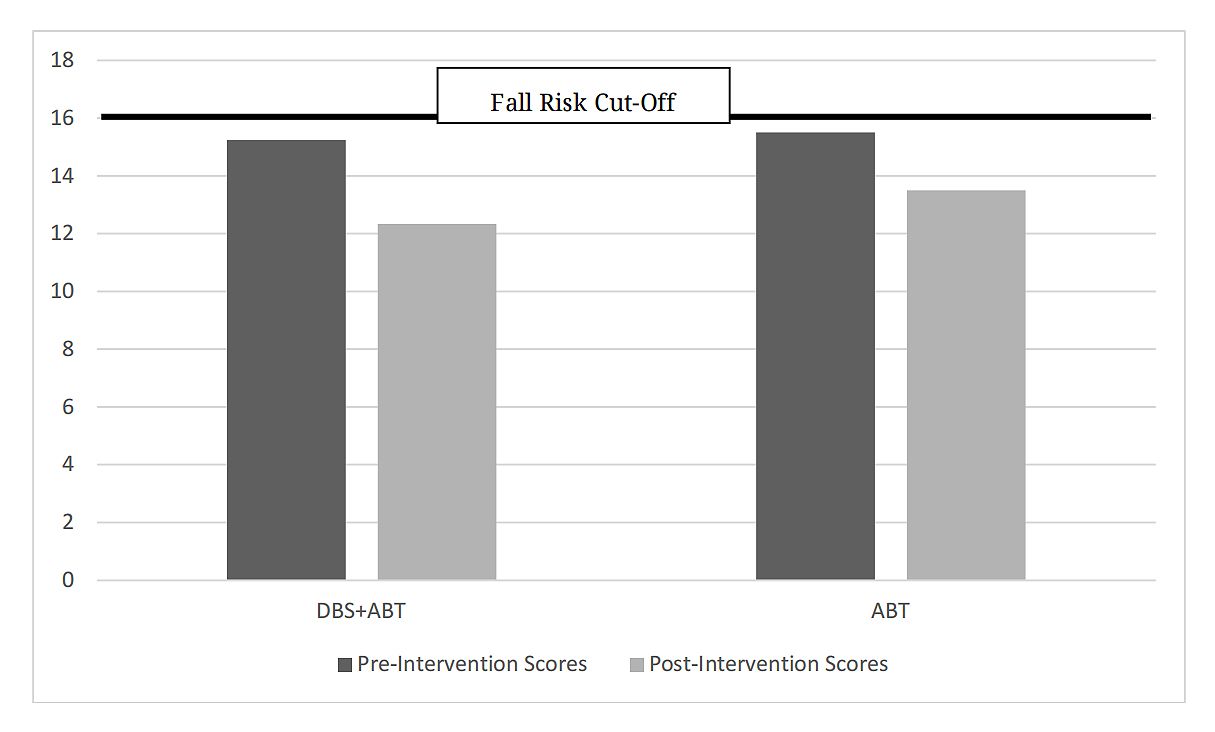 Figure 2. Five Times Sit to Stand Test times before and after Amplitude Based Training intervention.
Figure 2. Five Times Sit to Stand Test times before and after Amplitude Based Training intervention.
The results of the descriptive statistics showed that the DBS+ABT group had lower values for the TUG time difference before and after intervention (M = 1.17, SD = 1.59) than the DBS group (M = 4.14, SD = 3.58). The results of the descriptive statistics also showed that the post interventions TUG time for the DBS+ABT group (M = 8.93, SD = 1.98) and the ABT group (M = 9.86, SD = 6.41) make the cut off score of 20.0 seconds to be classified as independent for basic transfers, and cut-off score of 11.5 seconds to be classified as decreased fall risk based on mobility after the ABT intervention (Figure 3) [26].
The Levene test of equality of variance yielded a p-value of 0.096, which is above the 5% significance level. The Levene test was therefore not significant and the null hypothesis that all variances of the groups are equal was not rejected. Thus, there was variance equality in the samples.
A two tailed t-test for independent samples (equal variances assumed) showed that the difference between the two groups with respect to the TUG time difference before and after intervention was not statistically significant, t(11) = −1.87, p = 0.088, 95% confidence interval [−6.47, 0.52]. Thus, the null hypothesis was not rejected.
The effect size d was 1.04 (equal variances assumed). With d = 1.04 there was a large effect [25].
An interesting finding showed that if a one tailed t-test was performed, the DBS group has a smaller or equal value of the TUG time difference as the DBS+ABT group, and the result was statistically significant (t(11) = −1.87, p = 0.044). The ABT group has larger values than the DBS+ABT group for the TUG time difference.
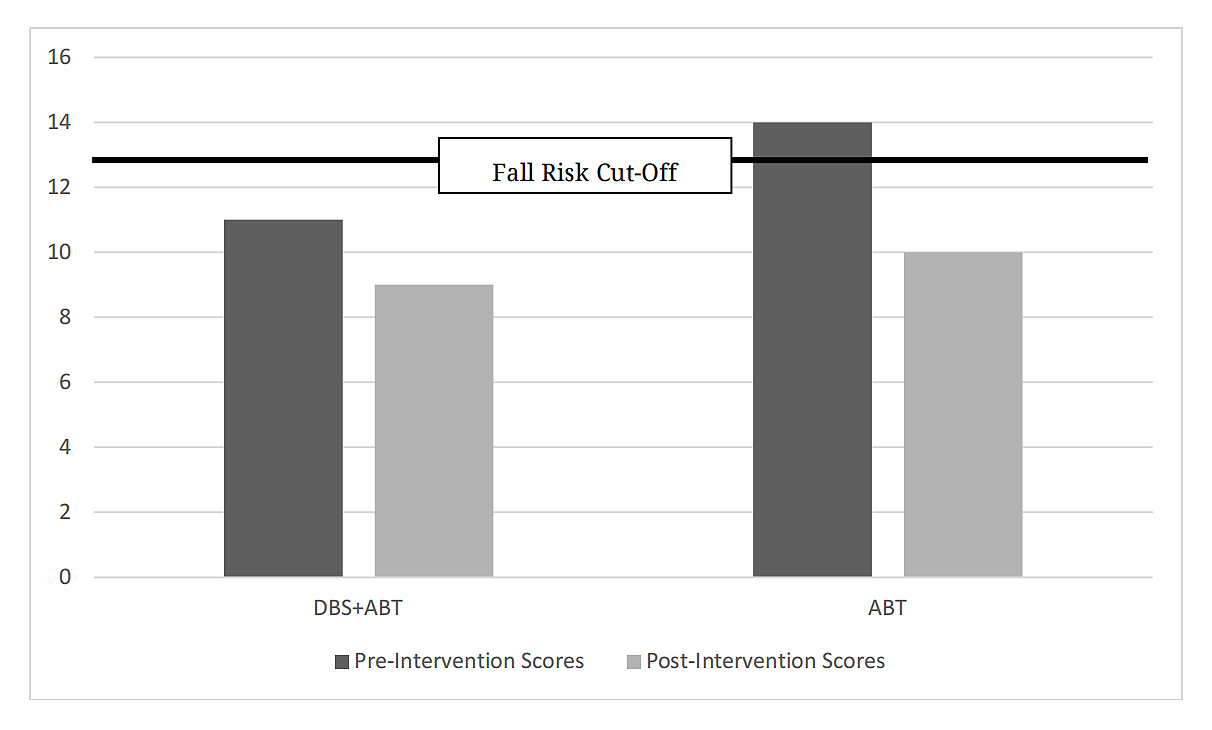 Figure 3. Timed Up and Go Test times before and after Amplitude Based Training intervention.
Figure 3. Timed Up and Go Test times before and after Amplitude Based Training intervention.
This is the first study looking at ABT in a population of PwPD who have had prior deep brain stimulation. The results of this study suggest that there is no significant difference in the results of ABT between individuals who have DBS and individuals who do not have DBS. This conclusion is based on measures of balance confidence, functional lower extremity strength, and general mobility. Clinicians may expect their patients with DBS to have similar outcomes as their patients without DBS when utilizing ABT.
The mean change in ABC-6 Scale score indicates similar improvements in balance confidence in both groups. Both groups had a mean post-intervention score at the ABC-6 Scale cut-off percentage score of 60%, meaning all patients were at the cutoff score and should still be classified as fallers because of their low balance confidence even after the ABT intervention [20].
The FTSST time difference pre and post intervention indicates an increased functional lower extremity strength in both of the groups. Both groups had mean post-intervention scores of less than 16.0 seconds indicating the individuals were classified as no longer a fall risk based on lower extremity strength after the ABT intervention.
The TUG time difference pre and post intervention indicates an improved general mobility in both of the groups. Both groups had mean post-intervention scores of less than 20.0 seconds indicating independence in basic transfers, and less than 11.5 seconds classifying the individuals having a decreased fall risk based on mobility post ABT intervention.
The results of this study generally support the hypothesis that each of the groups would have similar improvements on functional mobility outcomes after the ABT intervention. Several studies have explored the efficacy of amplitude-based training methods like LSVT-BIG for the PD population in general [12,27–30].
Future studies of this nature will be beneficial to explore this hypothesis under circumstances with fewer study limitations. The small all male sample of 14 participants significantly decreases the generalizability of the results. The retrospective design of this study exposes it to possible selection bias with convenience sampling. There were possible clinical factors that cannot be accounted for or controlled with a retrospective study design.
Future directions for research may include looking at similar aims with a larger sample size including all genders.
The results of this study indicate that there is no difference in the outcomes for individuals with DBS and individuals without DBS using ABT in functional outcomes of balance confidence, functional leg strength, and general mobility. Almost all participants in the study showed some improvements in each outcome measure, indicating that the intervention may be clinically useful in improving the mobility of PwPD.
The University of Central Florida Institutional Review Board determined this study design did not involve human subjects as defined by DHHS and FDA regulations (IRB #00001662). Patient consent was waived due to the retrospective design and IRB determination that it was not human subject research.
Declaration of Helsinki STROBE reporting guidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The dataset of the study is available from the authors upon reasonable request.
Conceptualization, MCB, RLB, KS, CS, CW, JT; Methodology, RL, AA, MCB, CS, CW, JT; Software, AA, MCB, RL; Formal Analysis, AA; Investigation, RLB, KS, LN, MCB; Data Curation, RLB, KS; Writing—Original Draft Preparation, CS, CW, JT, MCB, AA; Writing—Review & Editing, LN, AA; Visualization, MCB; Supervision, MCB; Project Administration, RLB, MCB.
Kathleen Salik reports she is an LSVT BIG Faculty but received no financial compensation for this research study. All other authors declare that they have no conflicts of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
Babcock RL, Anderson A, Neely L, Speranza C, Wilkerson C, Tolle J, et al. The Effects of Amplitude-Based Training on Mobility, Functional Leg Strength, and Balance Confidence in Persons with Parkinson’s Disease with and Without Deep Brain Stimulation: A Case Series. Adv Geriatr Med Res. 2025;7(2):e250006. https://doi.org/10.20900/agmr20250006

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




