Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(2):e250008 https://doi.org/10.20900/agmr20250008
 ,
Stuart Phillips 2 ,
Mike Grady 2
,
Stuart Phillips 2 ,
Mike Grady 2
1 LifeScan Global Corporation, 20 Valley Stream Parkway, Malvern, PA 19355, USA
2 LifeScan Scotland Ltd., Beechwood Park North, Inverness, IV2 3ED, UK
* Correspondence: Elizabeth Holt.
Background: Real-world evidence on technology use by older people with diabetes (PWDs) is sparse. We show that using the OneTouch Reveal® (OTR) diabetes app with Bluetooth® connected blood glucose meters improves diabetes management in older PWDs.
Methods: Anonymized glucose and app analytics from 160,545 PWDs, including 63,621 PWDs ≥65 years, were extracted from our server. Data from their first 14 days using the OTR app was compared with 14 days prior to a 180-day timepoint using paired within-subject differences.
Results: Data was retrieved from 133,817 people with type 2 diabetes (PwT2D; 78,167 <65 years and 55,650 ≥65 years) and 26,728 people with type 1 diabetes (PwT1D; 18,757 <65 years and 7971 ≥65 years). PwT2D ≥65 years improved blood glucose readings in range (RIR, 70–180mg/dL) at 180-days by +9.3 percentage points (%pts, 72.0 to 81.3%) and PwT1D improved by +5.2 %pts (60.6 to 65.9%). RIR progressively improved with higher app engagement in PwT2D ≥65 years, ranging from +7.2 %pts in those performing <1 app session per week to +11.4 %pts in those performing >10 sessions per week. RIR also progressively improved in PwT1D ≥65 years from +1.3 %pts with <1 session per week to +9.2 %pts in those performing >10 sessions per week. These glycemic changes were statistically significant (p < 0.001). The proportion of hypoglycemic readings remained largely unchanged.
Conclusions: Sustained improvements in glycemia showed progressive gains with stronger engagement with a diabetes app in PWDs ≥65 years, giving credence to the view that age is no barrier when using diabetes technology.
RWE, real-world evidence; OTR, OneTouch Reveal; OTVR, OneTouch Verio Reflect; OTVF, OneTouch Verio Flex; BGM, blood glucose meter; PWDs, people with diabetes; PwT2D; people with type 2 diabetes; PwT1D; people with type 1 diabetes; RIR, readings in range; RITR, readings in tight range; CGM, continuous glucose monitoring
The International Diabetes Federation estimates that the number of people with diabetes (PWDs) aged over 65 years could reach 195 million globally by 2030 [1]. In the US alone, a national survey estimated that nearly 30% of adults ≥65 years had diabetes [2], which is a concerning trend given that almost 25% of the US population is predicted to be ≥65 years by 2060 [3]. Most studies evaluating diabetes technology do not focus on older people [4], prompting a call to action for more studies in this population [5–9]. A recent review concluded that while technology eases the burden of self-care in older PWDs, age-related comorbidities can make technology use more difficult [10]. Recognizing this, the American Diabetes Association treatment goals for older PWDs are less stringent than for younger PWDs [11]. However, this does not imply that keeping blood glucose (BG) within safe levels is less important in older people. A recent study in people with type 2 diabetes (PwT2Ds) over 70 years of age found that maintaining A1c levels within a recommended range lowered mortality risk compared to A1c levels below or above range. This reinforces the need for tools that can support older PwT2D to keep their blood glucose levels within a safe range [12]. Older PwT2D manifest high rates of severe hypoglycemia [13], so it is especially important for them to benefit from technologies that help them recognize and act upon hypoglycemic readings.
Although improvements in technology and treatments have led to an increase in life expectancy for people with type 1 diabetes (PwT1D), recent global evidence highlights that optimal BG management, especially fasting BG, remains a major challenge for older people with T1DM [14]. Furthermore, it is postulated that advanced technologies, such as continuous glucose monitoring (CGM) and automated insulin dosing systems, that are popular in younger PwT1D may not be appropriate for many older people given that ageing may bring physical impairment and other challenges that hinder the use of technology [15]. Accessible, affordable and engaging digital therapeutics can play a key role in supporting diabetes management, as evidenced by their use in traditional clinical study designs that require PWDs to visit a clinical site in-person on multiple occasions [16–18]. However, real-world evidence (RWE) study designs that leverage information from far larger populations and do not involve clinical study sites can be a powerful way to substantiate the benefits of digital technology. To further this aim, and in light of the dearth of information regarding the benefits of diabetes technology in older people, we analyzed a large real-world dataset from PWDs who were using the OneTouch Reveal (OTR) diabetes app in combination with connected blood glucose meters (BGMs) to evaluate whether age presents a barrier to diabetes management and to what extent app engagement can affect glycemic outcomes.
Our dataset was drawn from PwT2D and PwT1D using the OTR diabetes app in conjunction with a Bluetooth connected OneTouch Verio Flex (OTVF) or OneTouch Verio Reflect (OTVR) BGM. These BGMs feature color range indicators that show if a current glucose reading is below range (blue), in range (green), or above range (red). After pairing the app to either meter, blood glucose readings automatically appear in the app (Figure 1). The app offers users colorful trends and easy tracking of glucose readings, the ability to annotate readings with food, activity or insulin dosing information, detection of low and high blood glucose patterns, and 14-day summary reports that may be especially helpful during consultations with healthcare providers, who have access to a professional version of the app where they can view the automatically transmitted data of their patients who have connected their OTR accounts to the healthcare provider’s clinic.
Our analysis dataset contained self-reported demographic information entered during app registration, including diabetes type, gender, date of birth and whether they used insulin. For this retrospective analysis, we used de-identified app data from the LifeScan server. A detailed description of how app data was collected and transferred to our server was published previously [19]. PWDs who downloaded the app were informed about the processing of personal data in accordance with the privacy policy, and they provided their explicit consent for this processing, which permits use of de-identified data to perform analytics, to conduct research and for product development. Additional ethics committee approval was not required, and no clinical sites or external investigators were involved. The current analysis fetched data from users who registered their app between January 2012 and March 2023.
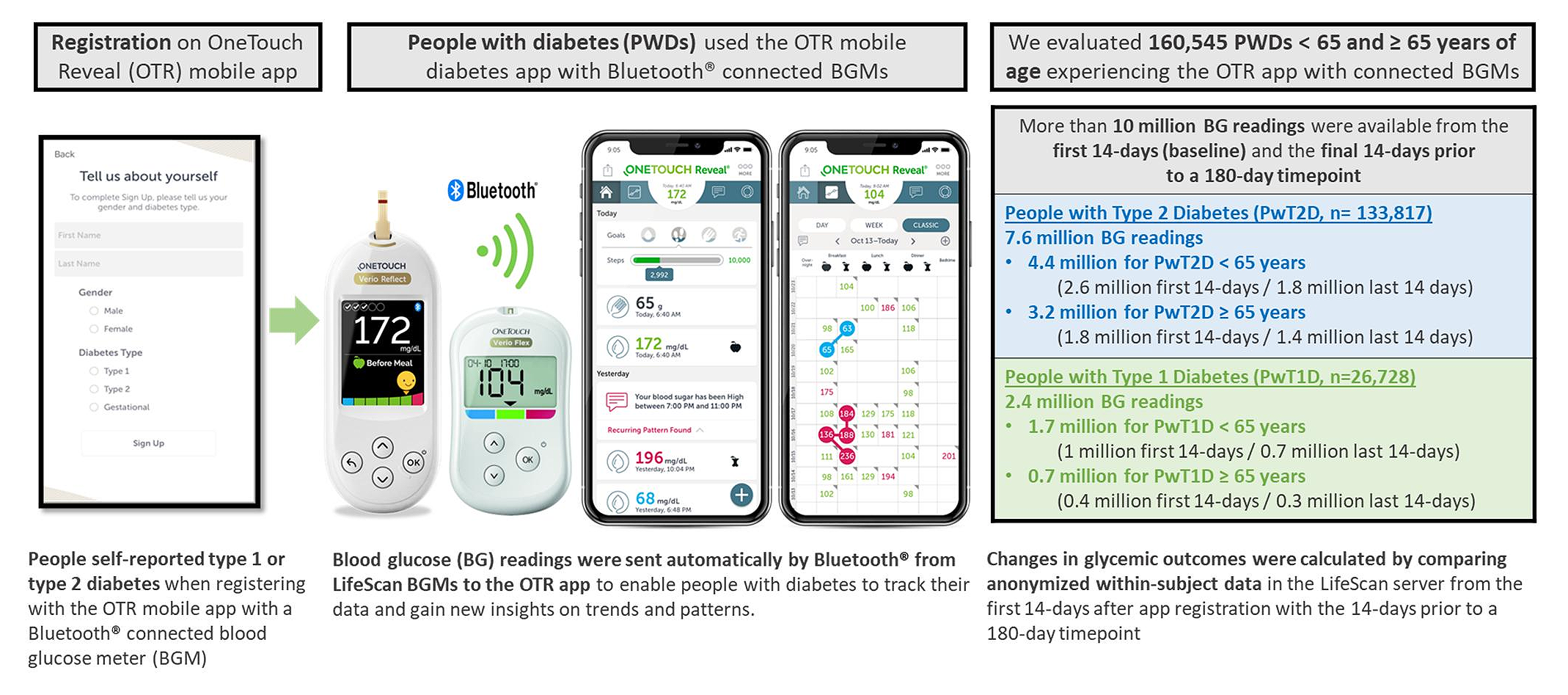 Figure 1. Process for real-world data collection from the OneTouch Reveal® mobile diabetes app.
Figure 1. Process for real-world data collection from the OneTouch Reveal® mobile diabetes app.
Analyses were performed for people who self-reported a diagnosis of type 2 or type 1 diabetes during app registration. People self-reporting a diagnosis of gestational diabetes were excluded. Our inclusion criteria required all subjects to have ≥180 BG readings over the first 180 days from the date of app registration. Glycemic data from each subject’s first 14 days using the app with their Bluetooth® connected BGM (baseline) was compared to the 14 days prior to each subject’s 180-day timepoint using paired, within-subject differences.
For each subject, the mean BG and percentage of readings within various glycemic ranges [hypoglycemic (<70mg/dL), readings in tight range (RITR, 70–140mg/dL), readings in range (RIR, 70–180mg/dL) and hyperglycemic (>180mg/dL)] were calculated for the first and last 14 days. Within-subject differences from baseline were then averaged across all subjects. App analytics were used to evaluate the influence of app engagement on glycemic outcomes. For each subject, the number of sessions and time spent in the app per week were averaged over the full 180 days. Categories of app usage were created based on the spread of the app engagement data over this timeframe; sessions per week were: <1, 1 to 2, >2 to 4, >4 to 10 and >10, and minutes per week on the app were: <2, 2 to 5, >5 to 10, >10 to 20, >20 to 40, >40 to 60 and >60. All statistical comparisons between baseline and the 180-day timeframe were performed using two-sample t-tests with SPSS Version 26.
Our retrospective analysis of BG readings and app analytics from 160,545 PWDs included a combined total of 10,073,110 BG checks using the OTVF or OTVR BGMs during the first 14 days after app registration and the 14 days prior to the 180-day timepoint. We did not include the BG readings between these timeframes. The dataset contained 133,817 PwT2D (78,167 <65 years and 55,650 ≥65 years) and 26,728 PwT1D (18,757 <65 years and 7971 ≥65 years) (Figures 1 and 2).
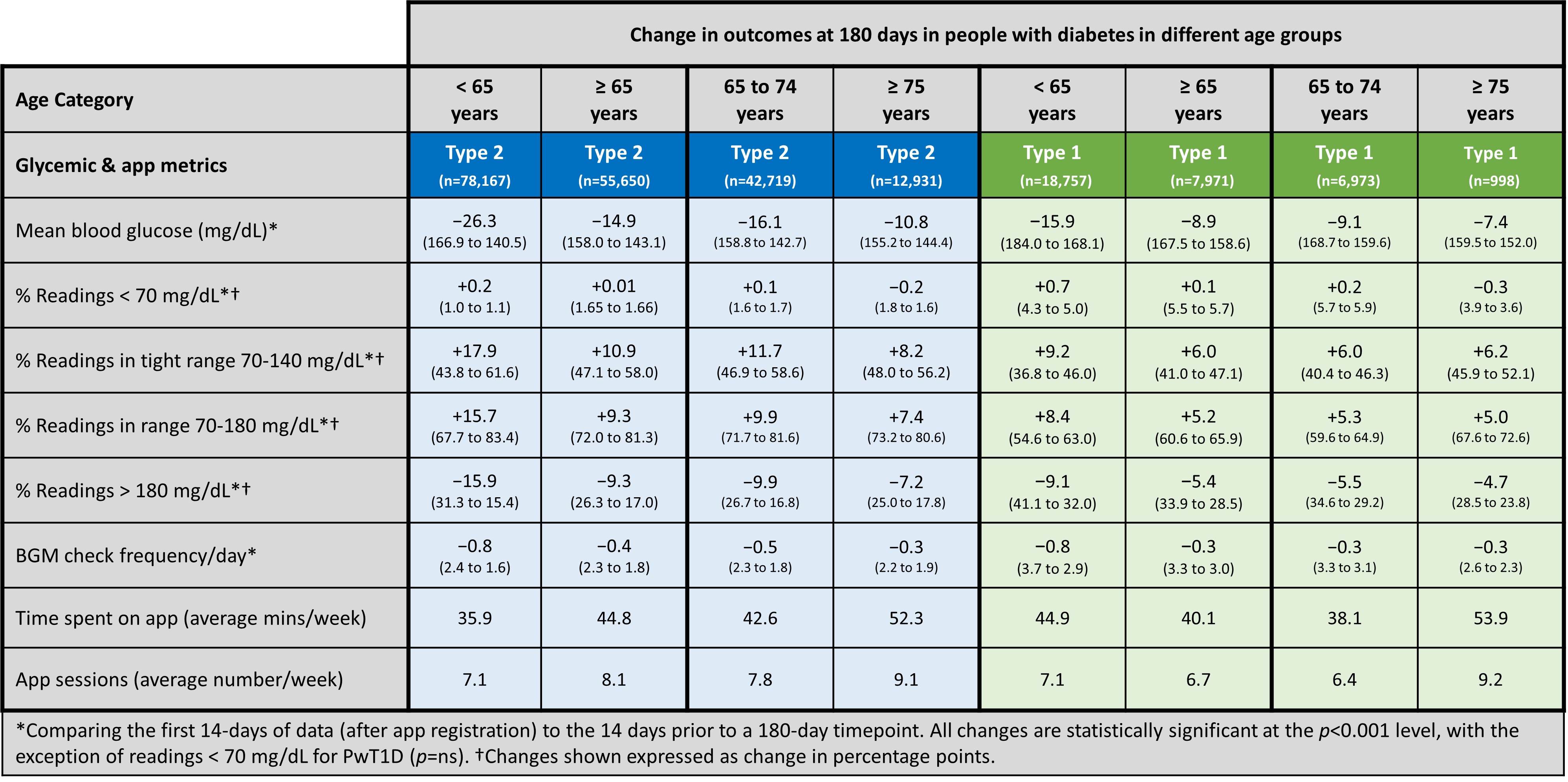 Figure 2. Summary of changes in outcomes at 180 days in people with diabetes in different age groups.
Figure 2. Summary of changes in outcomes at 180 days in people with diabetes in different age groups.
The outcomes achieved by different age groups in PwT2D and PwT1D are provided in Figure 2. Older PwT2D (aged ≥ 65 years) experienced clinically meaningful improvements in percentage of readings in range (RIR) of +9.3 percentage points (%pts) in comparison to a +15.7 %pt improvement in those <65 years. However, given that older PwT2D manifested a higher proportion of RIR at baseline, all age groups ultimately achieved more than 80% RIR at 180 days (83.4% in age < 65, 81.3% in age ≥ 65), with even the oldest PwT2D (age ≥ 75) reaching RIR of more than 80%. This oldest group of PwT2D invested more time exploring the app than the younger PwT2D (<65 years), spending approximately 16 minutes longer on the app per week (52 minutes vs 36 minutes).
Readings in tight range (RITR, 70–140 mg/dL)) is an important new metric that illuminates better glycemic management without crossing the hypoglycemia threshold. We observed a +10.9 %pt increase in RITR (47.1% to 58.0%) in PwT2D age ≥ 65, mirrored by both older PwT2D subgroups (ages 65 to 74 and ≥75). We also observed that readings < 70 mg/dL remained static (0.01 %pt change), despite PwT2D age ≥ 65 achieving +10.9 %pts more RITR. The driving force behind this tighter diabetes management was the marked reduction in hyperglycemic readings, which declined by almost −10 %pts in those aged 65–74, a category that represented approximately 77% of all those PwT2D aged >65 years.
We observed similarly positive trends in PwT1D. Older PwT1D (≥65 years) represented approximately 30% of our T1D cohort, and they improved RIR by +5.2 %pts in comparison to +8.4 %pts in PwT1D <65 years. We noted that the proportions of both RIR and RITR were lower in PwT1D compared to the equivalent age groups of PwT2D, with PwT1D aged ≥65 years achieving 66% RIR compared to 81% RIR in PwT2D. While PwT2D exhibited no clinically relevant increases in their hypoglycemic readings, PwT1D had no statistically significant or clinically relevant change in their percentage readings < 70 mg/dL while experiencing sustained glycemic improvements.
Impact of OTR App Engagement on Glycemic OutcomesWhile differences in degrees of improvement were seen in older compared to younger age groups and in PwT2D compared to PwT1D, engaging in more app sessions (or time on the app) per week progressively improved RIR for both older and younger PWDs and for both PwT2D and PwT1D. Glucose RIR in PwT2D performing 1 to 2 app sessions per week improved by +14.5 %pts in those aged <65 and by +6.9 %pts in those ≥65 years of age. PwT2D ≥65 years performing > 10 app sessions per week improved their RIR by +11.4 %pts (Figure 3). In contrast, PwT1D <65 years performing 1 to 2 app sessions per week improved their RIR by +6.0 %pts compared to +3.5 %pts in those ≥65 years. PwT1D ≥65 years performing >10 app sessions per week improved RIR by +9.2 %pts (Figure 4). The proportion of hypoglycemic readings remained largely unchanged with more app engagement in all the groups, even as RIR improved.
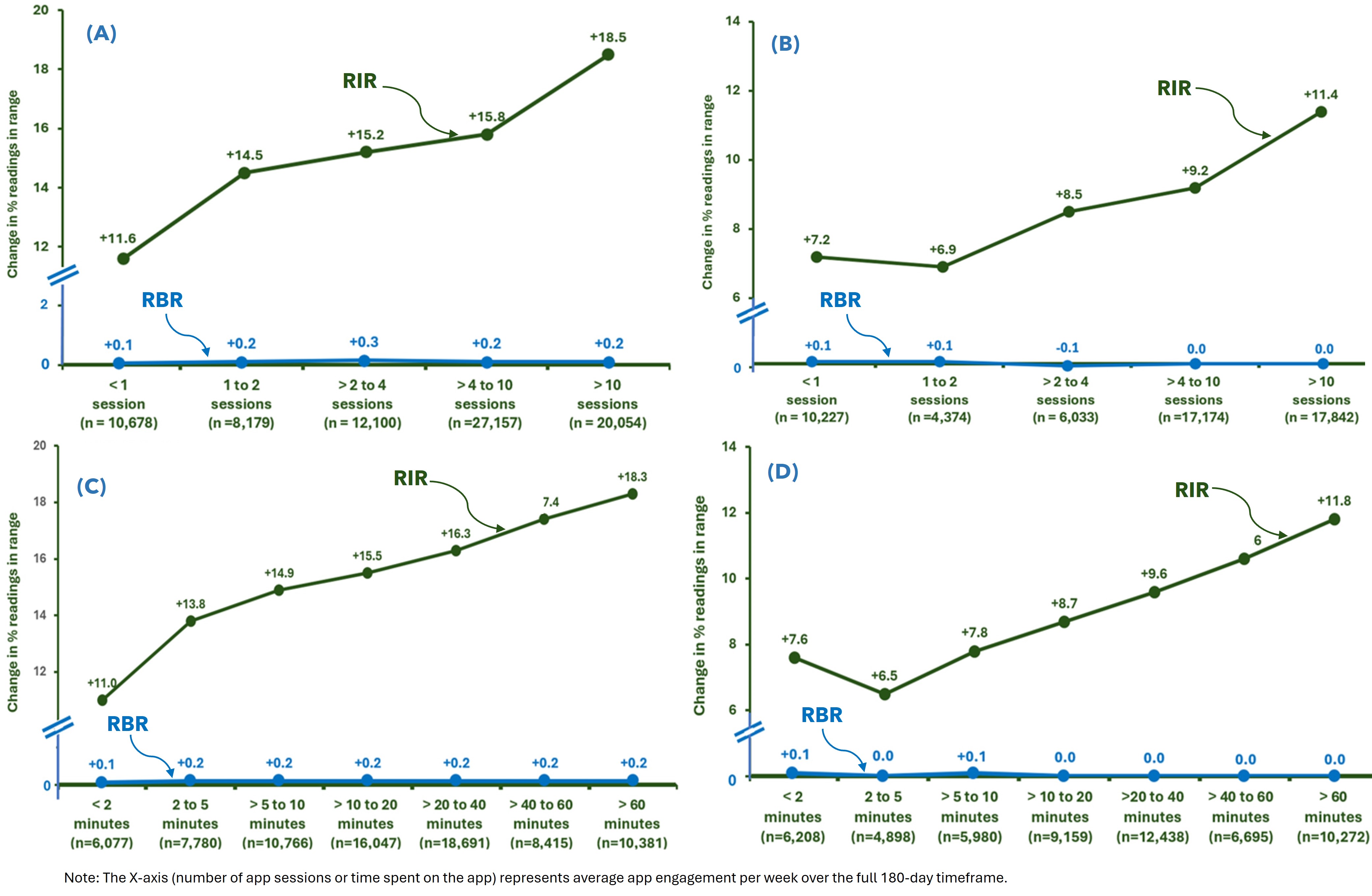 Figure 3. Improving glycemia with increasing app engagement in people with type 2 diabetes. (A) Type 2 < 65 years. (B) Type 2 ≥ 65 years. (C) Type 2 < 65 years. (D) Type 2 ≥ 65 years.
Figure 3. Improving glycemia with increasing app engagement in people with type 2 diabetes. (A) Type 2 < 65 years. (B) Type 2 ≥ 65 years. (C) Type 2 < 65 years. (D) Type 2 ≥ 65 years.
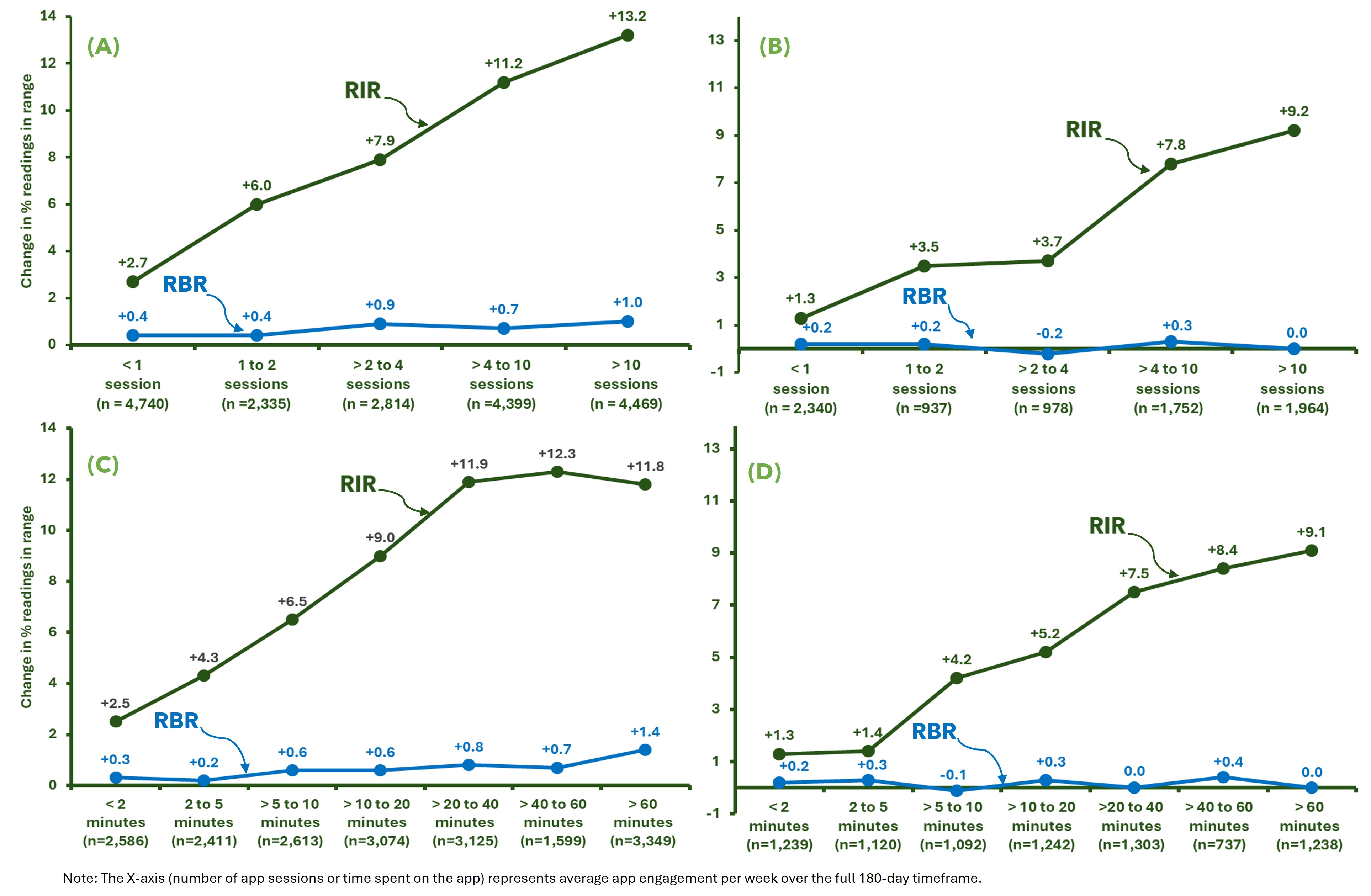 Figure 4. Improving glycemia with increasing app engagement in people with type 1 diabetes. (A) Type 1 < 65 years. (B) Type 1 ≥ 65 years. (C) Type 1 < 65 years. (D) Type 1 ≥ 65 years.
Figure 4. Improving glycemia with increasing app engagement in people with type 1 diabetes. (A) Type 1 < 65 years. (B) Type 1 ≥ 65 years. (C) Type 1 < 65 years. (D) Type 1 ≥ 65 years.
Additional analyses (See Supplementary File S1) provide more context on how people of different ages engaged with the app and how this influenced metrics other than RIR. The majority of PwT2D were highly engaged with the app, with 60.4% of those <65 years and 62.9% of those ≥65 years performing >4 app sessions per week on average over 180 days. In terms of time spent in app sessions, 48.0% of PwT2D < 65 years and 52.8% of those ≥65 years spent >20 minutes viewing app insights each week. Progressive improvements in mean BG mirrored trends of increasing app engagement in PwT2D. PwT2D <65 years who performed >2 to 4 app sessions per week lowered mean BG by −25.6 mg/dL from baseline at 180 days compared to a −13.2 mg/dL reduction from baseline for those ≥65 years of age. The change from baseline in the frequency of BG checking in each category of app engagement was similar in older and younger PwT2D. Similar trends and insights are reported for PwT1D, although, as stated previously, the magnitude of improvement in glycemic measures was lower for PwT1D than was observed for PwT2D.
Bluetooth connectivity of BGMs to diabetes apps has enabled retrieval of real-world data directly from people managing their diabetes at home at a scale that was not possible in the past. The availability, simplicity and intrinsic value of these consumer-friendly medical devices allowed us to compile an unprecedented dataset of BG readings and app analytics from more than 160,000 PWDs, of whom more than 63,000 were aged ≥65 years.
The importance of maintaining BG readings within safe glycemic ranges (classified as RIR or RITR) and avoidance of hypoglycemia, especially in the elderly, have become key areas of focus for diabetes management in recent years, and this new approach applies as much to data from BGM devices (readings in ranges) as it does to CGM devices (time in ranges). These new metrics have supplemented, if not superseded, the traditional focus of tracking patient progress via hemoglobin A1c measurements. Our data demonstrates a strong association between the initiation of our app/BGM ecosystem (as seen in Figure 1) and an improvement in readings in ranges at 6 months of home use. Importantly, these clinical benefits were achieved in the absence of any clinically worrisome increase in the percentage of hypoglycemic readings in older PWDs. For example, we observed that readings <70 mg/dL remained static (+0.01 %pt change) despite PwT2D age ≥ 65 achieving +10.9 %pts more RITR. In older PwT1D, who have been coping with diabetes over many decades, we observed no significant change in their readings <70 mg/dL (+0.1 %pts change, p = ns) while they achieved a 6.0 %pts improvement in their RITR.
Addressing interpretation and response to out of range BG readings has been identified as a prerequisite for diabetes management [20]. Despite this we previously reported that although nearly all PWDs would take action for low BG readings, 51% stated they would not take action for any level of high BG reading [21]. This was consistent with a study in PwT2D where only 28% of patients considered results >235 mg/dl as high, with a further 10% viewing only >290mg/dl as high [22]. This demonstrates a tolerance (or lack of awareness) of high BG levels in PwT2D. These findings previously prompted us to design on-meter and app-based features to enable PWDs to quickly recognize out of range readings to motivate them to take action [23]. It is conceivable that these (ColorSure® and Blood Sugar Mentor®) features in the meters and app used in our RWE study were partly responsible for improving readings in range. Our glucose monitoring systems are used worldwide by PWDs of all ages and, therefore, we felt it was important to contrast the outcomes achieved by older PWDs (≥65 years) with those of younger PWDs. Although the magnitude of improvement in percentage points was greater for RIR and RITR at 6 months of usage of the app/BGM ecosystem for those <65 years, older people had a similar overall proportion of readings in ranges at 6 months because they started with a higher proportion of RIR at baseline, with subsequently less room for improvement. While it is encouraging that older PWDs had similar glycemic outcomes to younger PWDs in our dataset, we recognize that these groups may differ in their lifestyles, activity levels, cognitive abilities, co-morbidities, diabetes duration and a host of other factors that confound direct comparison.
However, one area that is clear is the level of engagement with technology shown by older PWDs in our study. Many PWDs purchase (or an HCP provides them with) a new meter without training on its use, yet they were able to set up their devices at home, often customizing advanced settings or features. OneTouch BGMs are equipped with on-meter and in-app features, such as color range indicators, meal tagging options, pattern detection and even a blood sugar mentor tool that offers pop-up insights on the OTVR meter screen, all of which could have benefited the 63,000 older PWDs in our dataset.
Furthermore, we could not have retrieved data from older (or younger) PWDs if they had not first downloaded the OneTouch Reveal diabetes app, followed by syncing the app to one of our BGMs. It is important to acknowledge that these steps did not present an insurmountable barrier to these older people, so healthcare providers should have confidence when recommending connected devices and apps to older PWDs. It was also evident that app engagement was far higher in these older PWDs, regardless of diabetes type, but it is also perfectly reasonable to speculate that older users spent more time exploring the app, so it does not necessarily mean they were more engaged. Perhaps many older users simply required more time to analyse app data before making therapeutic or lifestyle decisions. Nonetheless, we clearly observed from the data that more interactions with the app were strongly associated with progressively more readings in range.
By their very nature, digital technologies, such as smartphones with apps, are intended for communication and bringing people closer together. In our study, it is conceivable that PWDs felt more connected to their HCPs when using the app, thus improving outcomes by fostering greater adherence to therapy. In fact, an important feature of the app enables PWDs to share 14-day progress reports directly with clinicians either face-to-face or remotely by text or email. Such tools may facilitate a stronger partnership with HCPs, ultimately improving patient adherence and outcomes.
This strong link between app engagement and improving glycemia combats a number of criticisms often levelled at RWE studies, where there is a lack of specific knowledge of the medical care or treatment changes that occurred during the data collection period. These factors could confound RWE studies on the benefit of an app, but the strong association we observed between progressively more app engagement and progressively better glycemic outcomes is plausibly a firm indication that this specific app/BGM ecosystem has a clinically meaningful impact over and above routine care. A recent systematic review provided a comprehensive summary of digital health solutions that concluded digital therapeutics can effectively improve A1c in PwT2D and that integration of digital health care into usual care holds great potential [24].
The continued adoption of CGM in diabetes management has provided great clinical and quality of life benefits, not least of which is the reassurance of alerts or alarms for impending hypoglycemia. The advantages of CGM, especially for PwT1D, are self-evident but it is also apparent that many older PWDs may not need a CGM, will not have access to CGMs, may not wish to wear CGMs continuously or, in some cases, may feel the data is overwhelming [25]. In addition, in outcome studies where apps and a connected BGM were compared to CGM, and in a meta-analysis [26] of BGM compared to CGM, the superiority of CGM, in terms of A1c reduction, has been limited. Bergenstal et al [27] found that, for PwT2D, the A1c outcomes achieved in the app/BGM group, who followed a structured BG monitoring schedule, were no different to the CGM group. Furthermore, a landmark study [28] in PwT2D comparing a Dexcom G6 CGM to the same app/BGM system (OTR/OTVF) used by many of the older PWDs in our dataset found that the app/BGM group lowered A1c by a credible −0.6% compared to −1.1% for Dexcom G6. These findings support use of an app/BGM ecosystem in PWDs without access to, or a desire to use, CGM, and for HCPs who are keen to offer an accessible, affordable glucose monitoring alternative to CGM with proven outcomes.
RWE studies often have access to patient-level clinical data, including deep knowledge of the subjects’ medical history, adherence to and/or changes in diabetes medications, the clinical goals set by HCPs, and measured A1c values. However, our study design was reliant on the more limited demographic information entered during app registration. Furthermore, we cannot verify the types of HCPs our cohort accessed or how often those HCPs used the app/BGM data during our data collection window to educate or advise PWDs or modify therapy. It is also unknown if subjects were offered CGM, while still continuing to use the app/BGM. Nevertheless, it is generally understood that CGM initiation largely ablates any BGM testing and this was not the case in our overall dataset.
Despite these limitations, there are multiple strengths of RWE studies compared to randomized controlled studies. Even the landmark randomized controlled studies that focused on diabetes devices (whether BGM or CGM) rarely recruited more than 250 PWDs (including the control group), used tertiary sites specializing in diabetes care, enrolled subjects who typically lacked diversity in terms of ethnicity, age, and socio-economic status, typically had long lists of exclusions for co-morbidities and, most critically to this analysis, often excluded older people. Our RWE design included more than 160,000 PWDs and was blind to such factors, given that we simply extracted day-to-day device interactions from PWDs of all ages in their usual settings, with only minimal exclusions, and knowing that a broad demographic, inclusive of PWDs covering all aspects of social determinants of health, were included. The widespread uptake of our diabetes app will enable us in the future to investigate outcomes, such as the influence of structured BG monitoring, and follow the course of diabetes management over time. Ongoing refinements to ensure we collect additional patient data during and after app registration will allow us to better understand the association between BG data and clinical measures.
Sustained improvements in glycemia showed progressive gains with stronger engagement with a diabetes app and an advanced Bluetooth® connected blood glucose meter in PWDs aged 65 years and older. These findings give credence to the view that age is no barrier when using diabetes technology.
The following supplementary materials are available online: https://doi.org/10.20900/agmr20250008, Supplementary File S1: Relationship between OTR app engagement and changes in study outcomes.
Ethical review and approval were waived for this study due to users providing consent for LifeScan to utilize their deidentified data during the app registration process per our privacy policy. Our privacy policy can be found at https://onetouchreveal.com/content/en_US/privacy. For this retrospective data analysis, we used de-identified data from our LifeScan server. Data was obtained from registered users of LifeScan’s OneTouch Reveal app. Users who download the app are informed about LifeScan’s processing of personal data in accordance with its privacy policy, and they provide their explicit consent for this processing, which permits LifeScan to use deidentified data to perform analytics, to conduct research and for product development. Additional ethics committee approval was not required, and no clinical sites or external investigators were involved. Regarding the Informed Consent Statement, informed consent was obtained from all subjects involved in the study.
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conceptualization, EH and MG; Methodology, EH and MG; Formal Analysis, SP; Data Curation, SP; Writing—Original Draft Preparation, EH and MG; Writing—Review & Editing, EH, SP and MG.
MG, SP, and EH are all current employees of LifeScan.
This research was funded by LifeScan Global Corporation.
We thank the users of the OneTouch Reveal app for sharing their deidentified health data to enable this analysis. The authors also thank Hilary Cameron for her initial statistical analysis of the server dataset.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Holt E, Philips S, Grady M. Older Age Is No Barrier to Improvements in Glycemia in People with Diabetes When Using a Diabetes App with a Bluetooth® Connected Blood Glucose Meter. Adv Geriatr Med Res. 2025;7(2):e250008 https://doi.org/10.20900/agmr20250008

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




