Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(2):e250010. https://doi.org/10.20900/agmr20250010
 ,
Nicole Dawson 2,* ,
Hannah Dawkins 2 ,
Emily Morrell 2 ,
Erica Rappleyea 2 ,
Holly Rogers 2 ,
Morris Beato 2
,
Nicole Dawson 2,* ,
Hannah Dawkins 2 ,
Emily Morrell 2 ,
Erica Rappleyea 2 ,
Holly Rogers 2 ,
Morris Beato 2
1 Physical Therapy, Select Physical Therapy, Kissimmee, FL 34744, USA
2 Division of Physical Therapy, College of Health Professions and Sciences, University of Central Florida, 12805 Pegasus Drive, Orlando, FL 32816, USA
* Correspondence: Nicole Dawson.
Background and Purpose: The global and individual impact of Parkinson plus syndromes and secondary parkinsonism requires more insight into the treatment and management of these conditions. Previous studies highlighted the benefits of amplitude-based training on persons with Parkinson disease. However, there is a lack of evidence on the effects of this intervention on persons with Parkinson plus syndromes and secondary parkinsonism. The purpose of this case series is to examine the impact of amplitude-based training exercises on the gait, functional strength, dynamic balance, and balance confidence of five individuals with Parkinson plus syndrome or secondary Parkinsonism.
Case Description: Five individuals were included in this case series including 3 subjects with vascular dementia with parkinsonism and 2 patients with multiple system atrophy.
Intervention: The individuals received amplitude-based training exercises four times a week for four weeks in an outpatient setting. Each session was 60 minutes in length and comprised seven standardized exercises focusing on movement amplitude. Training on four different activities of daily living, sit-to-stand transfer, and gait training were also included in every session.
Outcomes: All the participants showed improvement in outcome measures for gait speed, functional lower extremity strength, dynamic balance, and balance confidence with several individuals exceeding the minimum detectable change.
Discussion: These findings highlight the success of amplitude-based training exercises in improving activity limitations and participation restrictions in persons with Parkinson plus syndromes, in particular those with vascular dementia with parkinsonism and multiple systems atrophy.
Ten million individuals worldwide are currently estimated to be living with Parkinson disease (PD) [1]. The number of individuals diagnosed with PD is predicted to increase to over 1.2 million cases in the United States by 2030. In addition to those presenting with idiopathic PD, many present with what is termed secondary parkinsonism, in which other disorders have features similar to PD but have a specific etiology [2]. Vascular dementia with parkinsonism belongs to this classification and is caused by vascular lesions from small strokes. Although the pathophysiology of vascular dementia has not been widely studied, multiple studies have determined that a vascular infarct or stroke can cause white matter lesions and lacunes in the brain leading to lower extremity parkinsonian symptoms [3]. Some neurodegenerative conditions, known as Parkinson plus syndromes (PPS) mimic the clinical presentation of PD or secondary parkinsonism. These PPS, such as dementia with Lewy bodies (DLB), progressive supranuclear palsy (PSP), multiple systems atrophy (MSA), and corticobasal degeneration (CBD), manifest the constellation of motor symptoms of parkinsonism but include specific clinical features generally not seen in idiopathic PD [4,5]. These group of disorders present differently from PD with disease characteristics such as a faster disease progression, poor response to dopaminergic medications, lack of resting tremor, symmetric distribution, supranuclear gaze palsy, early postural instability, early dementia, asymmetrical apraxia, apraxia and dysautonomia [4,5]. Many persons with PPS demonstrate classical presentation of parkinsonism such as rigidity, bradykinesia, and postural instability making it difficult to differentiate from idiopathic PD [6–8].
Rehabilitation professionals such as physical therapists play a key role in improving the functional mobility and activity limitations of people with movement disorders. Although there is a paucity of literature concerning the rehabilitation of PPS and secondary parkinsonism, the scientific literature supports physical therapy intervention to improve long-term motor performance in individuals with idiopathic PD [9,10]. Amplitude-based training (ABT) is a physical therapy intervention that focuses on high-amplitude movements that are trained repeatedly at a high intensity with increasing complexity, and it has been shown to improve motor performance in individuals with PD. These large amplitude movements are hypothesized to target the proposed pathophysiological mechanisms underlying bradykinesia and hypokinesia [11–13].
A single overlearned verbal or proprioceptive cue seen with the ABT exercise program is hypothesized to decrease cognitive load and mental effort [14]. Most ABT exercise programs use a standardized protocol consisting of sixteen one-hour sessions supervised by a certified trained clinician over four weeks. This protocol consists of whole body, large amplitude movements practiced as maximal-effort, daily exercises, functional mobility component tasks, and walking activities. The maximal-effort exercises are composed of seven different exercises performed either in seated or standing incorporating full body movements with external cueing from the physical or occupational therapist for greater amplitude of movement, as well as sit-to-stand transfers. Functional mobility and activities of daily living (ADL) tasks are designed to target the participants’ specific mobility and ADL deficits. The participants are instructed to perform walking activities using a large amplitude arm swing and step length. Additional mobility tasks that may be given are typically more complex multistep mobility tasks such as bed mobility training or instrumental ADL training [13].
A systematic review of ABT in persons with Parkinson disease (PwP) showed improvements in the Unified Parkinson Disease Rating Scale (UPDRS), Timed Up and Go (TUG), and 10 Meter Walk Test (10MWT) after completing the standard ABT protocol of sixteen 60-minute sessions [13]. A study consisting of community-dwelling PwP demonstrated significant improvement in the TUG, Timed Up and Go Cognitive (TUG-C), and Timed Up and Go Manual (TUG-M) after the standard sixteen 60-minute sessions of ABT [12]. One study comparing the effects on mobility of ABT, Nordic walking, and unassisted home exercise showed improvements in the UPDRS-III, TUG, and 10MWT with the ABT group was superior compared to the other interventions [14]. The ABT exercise program is believed to be beneficial to individuals with idiopathic PD due to the recalibration of movement during exercise training resulting in a carryover of the ability of PwP to self-cue large amplitude movements during daily performance of ADL and functional mobility tasks even after ABT training has ended [15].
Very few studies assessed the benefits of ABT on individuals with secondary parkinsonism or PPS. One case report focused on a 57-year-old individual diagnosed with DLB who completed the ABT protocol. Although the individual made improvements in the TUG, 30 Second Chair Stand Test, Mini-Balance Evaluation Systems Test, 6 Minute Walk Test (6MWT), and Timed 25-Foot Walk, the results of the ABT case report were inconclusive due to the participant’s lack of consistency in performing the intervention [16]. Another case report presented a 74-year-old male with a diagnosis of PSP who has undergone a four-week ABT exercise program [17]. Improvement in the UPDRS and Berg Balance Scale (BBS) surpassed minimum detectable change (MDC) while improvements in the 10MWT were noted. A case of a 68-year-old man with olivopontocerebellar atrophy, a variant of MSA, showed that 20 weeks of ABT resulted in improvements exceeding the MDC or minimum clinically important difference (MCID) in Functional Gait Assessment, Five Time Sit to Stand Test (FTSST), preferred gait speed and 9 Hole Peg Test [18]. This is the first case series to our knowledge that examines the impact on activity limitation and functional mobility domains of ABT in other types of parkinsonism such as secondary parkinsonism and PPS, in particular vascular dementia with parkinsonism and MSA. The purpose of this case series is to examine the effect of ABT exercises on the gait speed, lower extremity strength, dynamic balance, and balance confidence of five individuals with PPS and secondary parkinsonism.
Participants in this case series lived in the community and included four males and one female (mean age = 75.2 years). Three of the individuals had a medical diagnosis of vascular dementia with parkinsonism and the other two individuals had a diagnosis of MSA. All individuals reported a history of falls and were referred to outpatient physical therapy secondary to motor symptoms and activity limitations. Participants’ characteristics are summarized in Table 1.
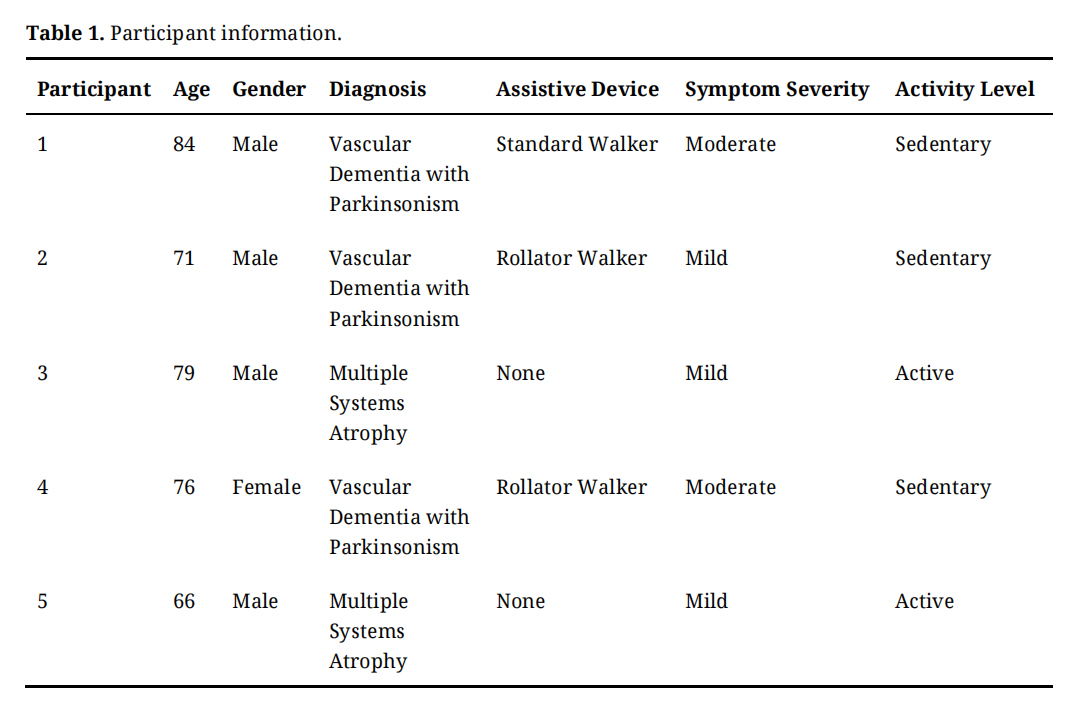 Table 1. Participant information.
Table 1. Participant information.
The outpatient physical therapy evaluation was standardized but was also designed for each individual’s clinical presentation, a specific variant of parkinsonism, and overall mobility.
The participant in Case 1 is an 84-year-old male who was diagnosed with vascular dementia with parkinsonism. The participant reported activity limitations and difficulty with ADL such as walking, cooking, dressing, and driving. He was identified as a fall risk and had difficulties with bed mobility and transfers. He was diagnosed with vascular dementia with parkinsonism less than a year before the initial physical therapy evaluation and he was referred to physical therapy secondary to balance impairment and falling. The participant reported a history of previous stroke with left-sided weakness, nocturia, and dysphonia. The prior level of function includes independent household ambulation without an assistive device. At the time of evaluation, the individual was using a standard walker for ambulation.
The participant in Case 2 is a 71-year-old male who was diagnosed with vascular dementia with parkinsonism. This individual was referred to physical therapy secondary to impaired balance and gait difficulties. He reported difficulty with mobility and ADL such as walking, upper body dressing, lower body dressing, and transfers. The participant experienced three falls before the physical therapy evaluation. The participant has a history of a previous stroke. The prior level of function includes being independent in basic ADLs. He used a rollator walker for household ambulation due to generalized weakness.
The participant in Case 3 is a 79-year-old male diagnosed with MSA. Physical therapy evaluation findings included impaired balance, bradykinesia, gait abnormality, difficulties with shower transfer, car transfers, and upper and lower body dressing. The participant reported a fear of falling. He was diagnosed with MSA one year before evaluation. This individual reported comorbid conditions such as diabetes mellitus, hypertension, hypothyroidism, cataracts, and lower extremity neuropathy.
The participant in Case 4 is a 76-year-old female with vascular dementia. Physical therapy evaluation findings include impaired mobility with sit-to-stand transfers, walking, and stair climbing. The patient also reported difficulty in upper and lower body dressing. She also reported resting tremors and postural hypotension. The individual was diagnosed with vascular dementia with parkinsonism one year before physical therapy evaluation. She was referred to physical therapy secondary to falling ten times in the previous year. The individuals’ medical history included anxiety, depression, headaches, hypertension as well as prior shoulder and hand injuries. The prior level of function includes independence with basic ADLs.
The participant in Case 5 is a 66-year-old male with MSA. He was diagnosed 2-3 years before physical therapy evaluation. He presented with impaired balance, micrographia, rigidity, freezing episodes during turning, and difficulty performing ADL tasks such as upper body dressing. In addition to his parkinsonism, the patient had a medical history of degenerative disk disease, prostate cancer, and a cardiac pacemaker implant. The patient’s prior level of function includes being fully independent with basic ADLs. Baseline outcome measure scores during physical therapy evaluation are listed in Table 2.
Based on the evaluation findings, the treating therapist determined an ABT exercise protocol would be appropriate for each of the patient’s conditions to increase the movement amplitude of upper extremity and lower extremity movements to improve activity limitations, functional mobility, and ADLs.
Tests and MeasuresThe specific outcome measures used include the Activities-Specific Balance Confidence Scale (ABC-6), Five Times Sit to Stand Test (FTSTS), Mini-BESTest, Timed Up and Go-Normal (TUG-N), TUG-C, TUG-M. Preferred gait speed and maximum gait speed were also measured with an assistive device listed in Table 1. Outcome measures were assessed at the initial physical therapy visit and at the completion of the ABT exercise protocol. The psychometric properties for the outcome measures have not been established in individuals with Parkinson Plus syndrome and secondary parkinsonism but will be compared to those assessed for persons diagnosed with idiopathic parkinsonism or PD where most of the psychometric properties have been established.
The ABC-6 is a shortened version of the 16-item self-reported full ABC Scale designed to assess a patient’s balance confidence while performing various activities. The ABC scale is a valid and reliable measure with excellent test-retest reliability (Intraclass correlation coefficient (ICC) = 0.94) and internal consistency (Cronbach’s Alpha = 0.95) [19].
The FTSTS is a performance measure used to assess functional lower extremity strength and sit-stand transfer. Psychometric properties for PwP include test-retest reliability (ICC = 0.76) and interrater reliability (ICC = 0.99) which are excellent [20]. An MDC value of 3.6–4.2 has been established with a cut-off score greater than 16 seconds indicating a high fall risk probability in PwP [20].
The Mini-BESTest is a 14-item clinical assessment tool used to assess dynamic balance. The test has excellent test-retest reliability (ICC = 0.92) and excellent interrater reliability (ICC = 0.91) for PwP [21]. An MDC value of 5.52 points has been established with a cut-off score of less than 20/32 demonstrating an adequate ability to predict fallers at both a 6-month and 12-month follow-up with patients with idiopathic PD [21].
The TUG-N is a performance measure easily administered and commonly used to assess general mobility and fall risk in a clinical setting. The test has excellent test-retest reliability (ICC = 0.80) and excellent interrater reliability (r = 0.99) in PwP [22,23]. An MDC value of 4.85 seconds has been established, and a cut-off score of greater than 16 seconds is significantly associated with an increased fall risk [22]. A cutoff score of 14.7 seconds for the TUG-C and 13.2 seconds for the TUG-M for fall risk has been previously established in persons with idiopathic PD [23,24].
Gait speed is a walking test to examine the speed of ambulation at both a comfortable pace and a maximum pace [16]. The test has excellent test-retest reliability (ICC = 0.96) for a comfortable gait speed and an excellent test-retest reliability (ICC = 0.97) for a maximum gait speed [25]. An MDC value of 0.18 m/s for the preferred gait speed and 0.25 m/s for the maximum gait speed has been established for PwP [26].
InterventionThe intervention followed a standardized four-week ABT exercise protocol. Standard dosing for typical ABT program is four sessions per week over four weeks. All sessions are 60 minutes in length and performed in a one-on-one manner with the physical therapist [13]. The clinician who administered the intervention was certified in ABT.
The participant in Case 2 was the only individual who deviated from the standard 16-session protocol, receiving an additional 6 sessions for a total of 22 intervention sessions. The plan was extended due to an illness during the administration of the regular protocol resulting in missed sessions. The protocol was extended to achieve the dosing of the intervention as determined by the treating physical therapist.
All the participants were given additional functional mobility or ADL tasks specific to the individual patient’s need which was determined by the patient and the physical therapist.
The participants all began the program following a thorough evaluation from a licensed physical therapist certified in ABT. A summary of the participants’ interventions is reported in Table 2. The patients were instructed to complete the same activities at home, once daily on physical therapy intervention days and twice on days not receiving intervention. Additional functional mobility tasks were assigned on a daily basis, which were specific to each patient’s deficits. Tasks were assigned based on activities the patient was already performing in their everyday life and they were instructed to perform these tasks at a high amplitude.
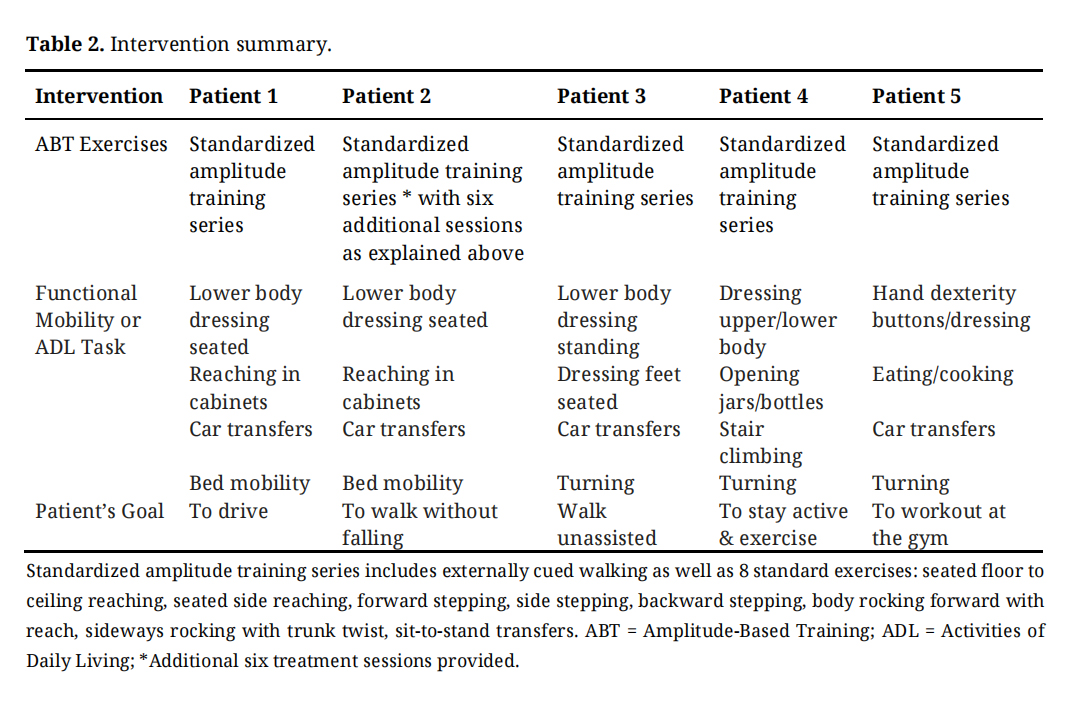 Table 2. Intervention summary.
Table 2. Intervention summary.
The results of this study indicated that each participant improved their scores in most of the outcome measures and reached an MDC in at least one of the outcome measures. The scores of each individual’s outcome measure at pre-test and post-test are reported in Table 3 and in Figure 1.
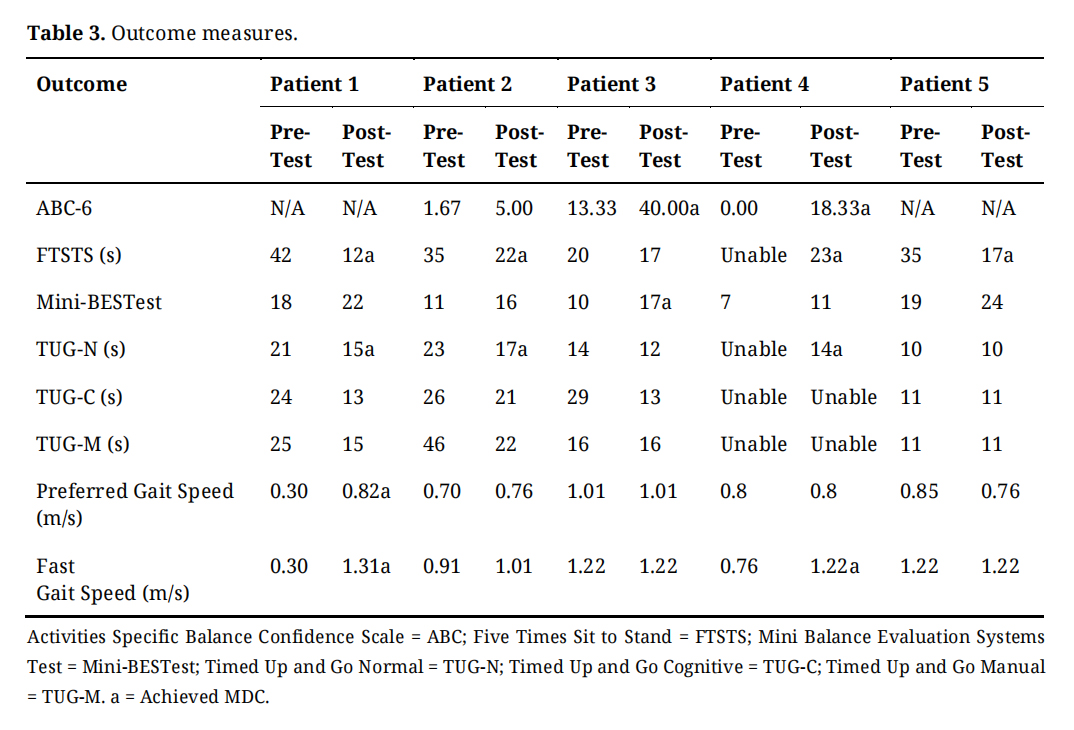 Table 3. Outcome measures.
Table 3. Outcome measures.
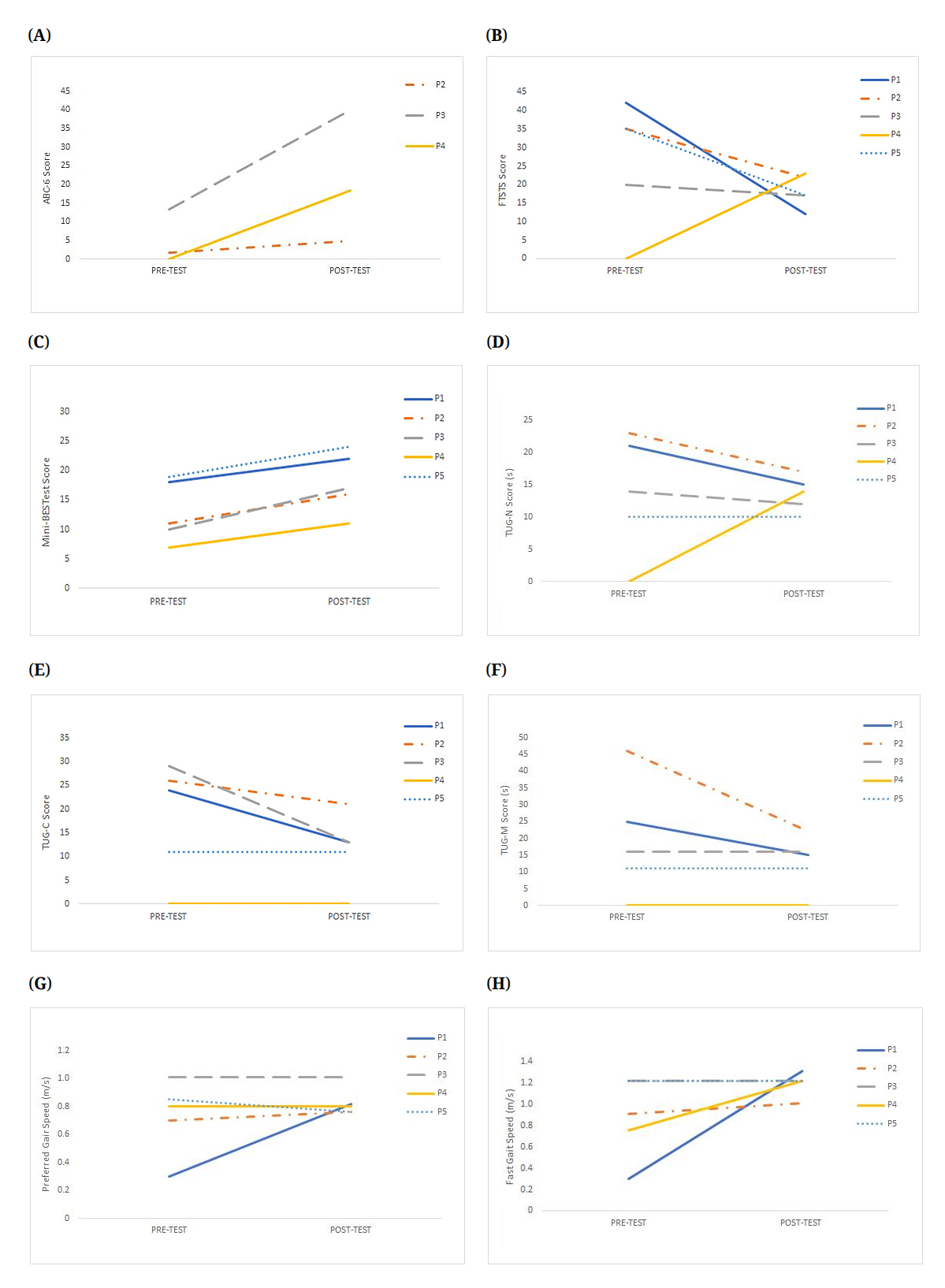 Figure 1. Changes between Pre-Test and Post-Test Outcome Measures. (A) ABC-6, (B) FTSTS, (C) Mini-BESTest, (D) TUG-N, (E) TUG-C, (F) TUG-M, (G) Preferred Gait Speed, (H) Fast Gait Speed.
Figure 1. Changes between Pre-Test and Post-Test Outcome Measures. (A) ABC-6, (B) FTSTS, (C) Mini-BESTest, (D) TUG-N, (E) TUG-C, (F) TUG-M, (G) Preferred Gait Speed, (H) Fast Gait Speed.
The participant in Case 1 demonstrated an improvement in the following outcome measures: FTSTS by 30 seconds, TUG-N by 6 seconds, preferred gait speed by 0.52 m/s, and fast gait speed by 1.01 m/s. The MDC was achieved in these four outcome measures. Improvements were also noted but MDC was not achieved in the following measures: Mini-BESTest by 4 points, TUG-C by 11 seconds, and TUG-M by 10 seconds. Based on established cut-off scores, improvement in his FTSTS, TUG-N, and Mini-BESTest classifies the participant’s score as a low fall risk after the intervention [20–24].
The participant in Case 2 demonstrated improvement in reaching MDC in the following measures: FTSTS by 13 seconds, and TUG-N by 6 seconds. Improvements were also noted but MDC was not achieved in the following measures: ABC score by 3.33 points, Mini-BESTest by 5 points, TUG-C by 5 seconds, TUG-M by 24 seconds, preferred gait speed by 0.06 m/s, and fast gait speed by 0.1 m/s.
The participant in Case 3 demonstrated improvement in reaching MDC in the following measures: ABC-6 by 26.67 points and Mini-BESTest by 7 points. Improvements were also noted but MDC was not achieved in the following measures: FTSTS by 3 seconds, TUG-N by 2 seconds, and TUG-C by 16 seconds.
The participant in Case 4 demonstrated improvement in reaching MDC in the following measures: ABC-6 by 18.33 points, FTSTS by 23 seconds, Mini-BESTest by 11 points, TUG-N by 14 seconds, and fast gait speed by 1.22 m/s.
The participant in Case 5 demonstrated a score improvement and achieved MDC for FTSTS. Improvements were also noted but MDC was not achieved in the Mini-BESTest by 5 points. Based on the established cut-off scores, the participant in Case 5 improved the Mini-BESTest score classifies the individual at a low fall risk following the ABT intervention [21].
The participants with PPS and secondary parkinsonism were all able to participate and complete the full ABT exercise protocol for this case series. All five individuals benefited from the ABT intervention and showed improvements in multiple domains of mobility post-intervention including dynamic balance, general mobility, functional lower extremity strength, balance confidence, and gait speed. While this study focused on the effects of ABT in individuals with PPS type of parkinsonism, the findings of this study coincide with the results from another study showing that ABT exercises improve motor function in idiopathic PD [11]. The results of this study are also similar to the findings of multiple studies showing that ABT exercises improve general mobility measured by the TUG performance in individuals with idiopathic PD [12–14]. The improvement in balance of the individuals in this case series is similar to the findings of improved balance in an individual with PSP using ABT exercises [17]. The improvement in leg strength of the individuals in this case series is similar to the results showing improved performance in the FTSST in a case study of an individual with olivopontocerebellar atrophy type of MSA [18]. This case series demonstrates that the use of an ABT exercise protocol by an ABT-certified physical therapist on patients with vascular dementia with parkinsonism and patients with MSA may potentially improve the individuals’ balance confidence, dynamic balance, functional lower extremity strength, gait speed, and general mobility. This case series additionally supports the research available on the benefits of using ABT for persons with any type of parkinsonism: be it idiopathic, PPS, or secondary [11–18].
The results of this case series may be beneficial and applicable to patients who are affected by parkinsonism, their caregivers, rehabilitation professionals, and movement disorder specialists due to the improvements in functional mobility and decreased risk of falls in the participants of the study. Rehab clinicians experienced in idiopathic PD may be already be familiar with ABT and may already use this technique with treating PwP. These same clinicians may not be as familiar or confident in treating individuals with PPS and secondary parkinsonism as these conditions are far rarer than idiopathic PD with significantly less robust supportive evidence on interventions that are effective in these individuals. The authors hope that the results of this study will begin to provide clinicians the confidence to treat these rarer conditions effectively by adapting the interventions they may already be using in PwP for use in individuals with other forms of parkinsonism.
There are several limitations to this case series. The data was retrospectively collected and only a small number of individuals were included in this study. The patient population in the case series is homogenous in terms of age and gender being limited primarily to older men and may not be reproducible in younger patients and women with atypical parkinsonism. It is less likely that a small homogenous sample will capture the diversity and generalizability of the findings to the larger population with PPS. Our study included more men than women perhaps as the prevalence of MSA of 2.75 per 100,000 for men is slightly higher than the prevalence of 1.19 per 100,000 for women [27]. The prevalence of vascular dementia is also equal for both men and women [28]. Additionally, this case series only examined patients with vascular dementia with parkinsonism and MSA, and did not include other types of PPS such as PSP or CBD or other causes of secondary parkinsonism. Further research needs to expand to other types of parkinsonism to determine if ABT intervention will also be an effective intervention in other forms of parkinsonism. Comparison studies of ABT programs versus “standard” care or no intervention may help add rigor to future studies. Finally, additional points of assessment (e.g., weekly or biweekly) may add in gaining a better understanding of the trajectory of progress and gains made during the intervention.
This case series is the first study to the authors’ knowledge that shows positive results that a standardized ABT exercise protocol is beneficial in persons with Parkinson plus syndrome and secondary parkinsonism. The results indicated that in persons with vascular dementia with parkinsonism and MSA, ABT may improve the individuals’ functional lower extremity strength, dynamic balance, gait speed, general mobility, and balance self-confidence. Further research is needed to generalize the results found in this case series and to ensure that the ABT protocol is effective in other types of Parkinsonism. Future research should include a larger number of subjects to increase the external validity of this study for this patient population.
The study was deemed “non-human subjects research” by the Institutional Review Board of University of Central Florida (protocol code STUDY00001662).
The dataset of the study is available from the authors upon reasonable request.
Conceptualization, RB, ND, HD, EM, ER, HR and MB; Methodology, MB, RB, ND; Formal Analysis, RB, MB; Resources, MB, RB; Data Curation, RB, HD, EM, ER, HR; Writing—Original Draft Preparation, RB, MB; Writing—Review & Editing, RB, ND, HD, EM, ER, HR and MB; Visualization, RB; Supervision, ND, MB; Project Administration, RB, MB.
The authors declare that they have no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Babcock R, Dawson N, Dawkins H, Morrell E, Rappleyea E, Rogers H, et al. Amplitude-Based Training in Secondary Parkinsonism and Parkinson Plus Syndrome: A Case Series. Adv Geriatr Med Res. 2025;7(2):e250010 https://doi.org/10.20900/agmr20250010

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




