Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250019. https://doi.org/10.20900/agmr20250019
 ,
Helene Støttrup Andersen
,
Helene Støttrup Andersen
Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense 5230, Denmark
* Correspondence: Jesper Bo Nielsen
Background: From about age 50, the prevalence of diseases begins to increase along with other life-changing decisions, both in general and within the health domain. Understanding the associations between individual characteristics that influence behavior and domain-specific risk-taking propensity is important but remains scarcely studied among older adults.
Methods: A cross-sectional survey on risk propensity based on a representative group of 7232 Danish citizens aged 51–80 years. Risk-taking propensity was the outcome, and questions were based on the German Socio-Economic Panel Studies (SOEP) and focused on the general and the health domains, respectively. Variables included sex, age, smoking status, alcohol consumption, BMI and questions related to individual characteristics. Analyses were based on chi-square and logistic regression.
Results: Within the group of older adults, a significantly higher fraction of respondents reports a high risk-taking propensity when framed in the general risk domain (23%) than in the specific health risk domain (4%). In our sample of respondents above 50 years, modifiable lifestyle-related variables (smoking, alcohol intake, BMI) were the only significant determinants of risk-taking propensity within the health domain.
Conclusion: Our findings challenge conclusions from previous studies on older adults’ priorities and behavior in the health domain when based on an unspecific risk framing, as older adults appear 5–6 times more reluctant to take risks if the setting is within the specific health risk domain compared to unspecific settings. Further, our study confirms the importance of including lifestyle-related variables in studies on risk-taking propensity of older individuals.
Most people make decisions of importance for their health and well-being every day. Some are well-considered, others are more intuitive, but all are based on individual values, preferences, priorities, and eventually adding up to a propensity to act in a specific way. This paper demonstrates how some risk-related lifestyle or behavioral characteristics, present health status, and expectations for the future are reflected in stated risk-taking propensities among older adults generally as well as within the health domain. The perspective is that a better understanding of the dynamics including age and sex of individual risk-taking propensities will allow for more targeted preventive initiatives towards modifiable lifestyle-related risk factors.
Risk propensities have been associated with lifestyle choices as well as more behavioral characteristics [1–4]. Much research on risk propensity has been on individuals from their teenage years to early adulthood in their thirties [1,5–7]. A period in life with significant changes in many domains of life including risk-taking propensities. However, from about age 50 and upwards, where the prevalence of diseases begins to increase together with other life-changing decisions, knowing more about associations between individual characteristics of importance for behavior and risk propensity seems equally important, but much less studied [8]. The present study will focus on people of 51 to 80 years of age.
Expectations for the future, anxiety, and the wish to plan in good time are probably parts of the same personality construct. We would expect a fair agreement (co-variance) between them. There is a significant age gab in expectations for the future between people below 30 and those above 50 years-of-age [9], the incidence of anxiety disorders is significantly lower among people above 50 years-of-age [10], and the fraction of the population being above 60 years-of-age has grown markedly in most countries and is expected to continue growing [11]. Knowing that the older a person gets, the more concrete and time-limited the future will be, it appears relevant to study how risk propensity is associated with an individual’s perspectives of a future that is shorter than the life lived up till now—especially related to the health domain as disease prevalence generally increase with age.
Several constructs have been developed to measure risk propensity, and they often use a Likert or similar scale to quantify the stated propensity [1]. The majority of the population studied is expected to belong to the central part of the distribution, but from a preventive perspective it is probably the smaller groups covering the extremes that are most interesting. We therefore focus on respondents with either high or low stated risk aversity, rather than on the mean propensity.
The present study aims at discussing associations between risk taking propensity and individual lifestyle and behavioral characteristics based on three decades of older Danish adults (age 51–80), and with a focus on characterizing associations observed within the fractions of the populations with lowest or highest risk-taking propensities. We expect that stated risk-taking propensity will be significantly associated with lifestyle variables (smoking, alcohol consumption, BMI) as well as individual characteristics such as anxiety and expectations for the future with a potential dependency on respondents’ age.
We used a cross-sectional survey design based on a representative group of 15,072 Danish citizens aged 51–80 years. Data was collected in 2019 through a web-based standardized questionnaire (digital mail) administered by Statistics Denmark. Two reminders were sent through digital mail. Among the net sample, 7232 persons (48%) returned a questionnaire covering topics related to risk propensity.
Risk taking propensity was the outcome variable, assessed in both general and health domains based on questions originally developed and used in the German Socio-Economic Panel Studies (SOEP, www.leibniz-soep.de accessed on 10 Jun 2025). Answers were given on an eleven-point Likert scale, and in this paper a low risk-taking propensity is defined as answering 0, 1, or 2 on the Likert scale, and a high risk-taking propensity is defined as answering 8, 9, or 10 on the Likert scale (cut-off points chosen to represent low and high quartiles).
As variables we included sex (female, male), age (51–60, 61–70, 71–80 years-of-age), smoking (yes, no—quit, never), weekly alcohol intake (0, 1–7, 8–14, 15–21, >21 drinks), body mass index (BMI <25, 25–30, >30), feeling well enough to do what you like to do (yes, always or mostly; yes, sometimes; No, rarely or never), expecting to live longer than others with same sex and age (yes, no, don’t know), feeling anxiety or depression (no, little or moderate, very or extreme), satisfaction with own health (Likert scale; 0–6, 7–8, 9–10), and planning in good time (Likert scale; 1–3, 4, 5, 6).
Statistical AnalysisFor both health and general risk propensity, population characteristics were presented as n (%). For bivariate analyses, a chi-square test was used to test for independence between characteristics and high or low risk-taking propensity. A logistic regression with robust standard errors was used to see the association between population characteristics and risk-taking propensity. Results were presented as odds ratios (OR), 95% confidence intervals, and p-values. p-values < 0.05 were considered statistically significant. Lastly, a correlation matrix was presented.
All analyses were conducted using Stata version 18 (StataCorp LP, College Station, TX, USA).
Among the 7232 respondents, 833 (11.5%) stated a low and 1691 (23.4%) a high risk-taking propensity within the general risk domain, respectively (Table 1). Within the health domain, the equivalent numbers for the same group of respondents were 3829 (52.9%) for a low and 300 (4.1%) for a high risk-taking propensity, respectively (Table 1).
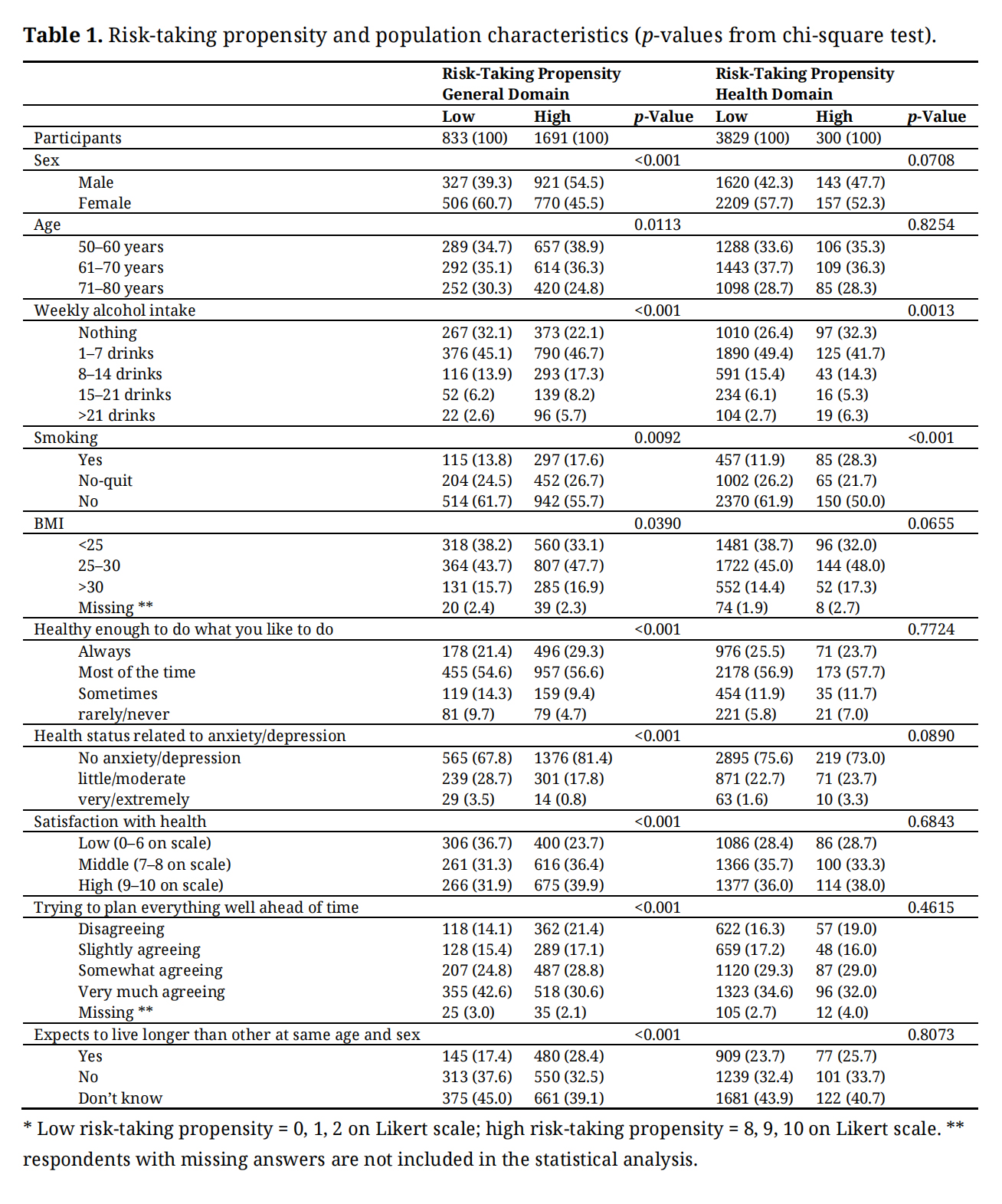 Table 1. Risk-taking propensity and population characteristics (p-values from chi-square test).
Table 1. Risk-taking propensity and population characteristics (p-values from chi-square test).
Among respondents with a high risk-taking propensity in the general risk domain women and the oldest age group of respondents (71–80 years) were significantly less represented. Weekly alcohol intake, smoking, and BMI were all significantly associated with stating a high general risk-taking propensity. Further, respondents being sufficiently healthy to do what they like to do, not feeling anxiety or depression, being satisfied with their health, not planning everything well ahead of time, and expecting to live longer than others were all associated with stating a high risk-taking propensity within the general risk domain in the bivariate analyses (Table 1).
Focusing on risk taking within the health domain, neither sex, age, nor psychosocial variables were statistically associated with low or high risk-taking propensity (Table 1). The only variables positively associated with high risk-taking propensity within the health domain were weekly alcohol intake and smoking (Table 1).
The regression models for the general risk-taking propensity as well as the risk-taking propensity within the health domain confirmed the initial bivariate analyses. Thus, the general risk-taking propensity was higher for males, for those drinking alcohol, for those with a BMI > 30, for smokers, those expressing satisfaction with health status, and for those with a self-rated higher life expectancy than their peers (Table 2). In contrast, respondents above age 70, respondents with stated planning behavior, and respondents reporting symptoms of anxiety or depression stated a lower general risk-taking propensity (Table 2).
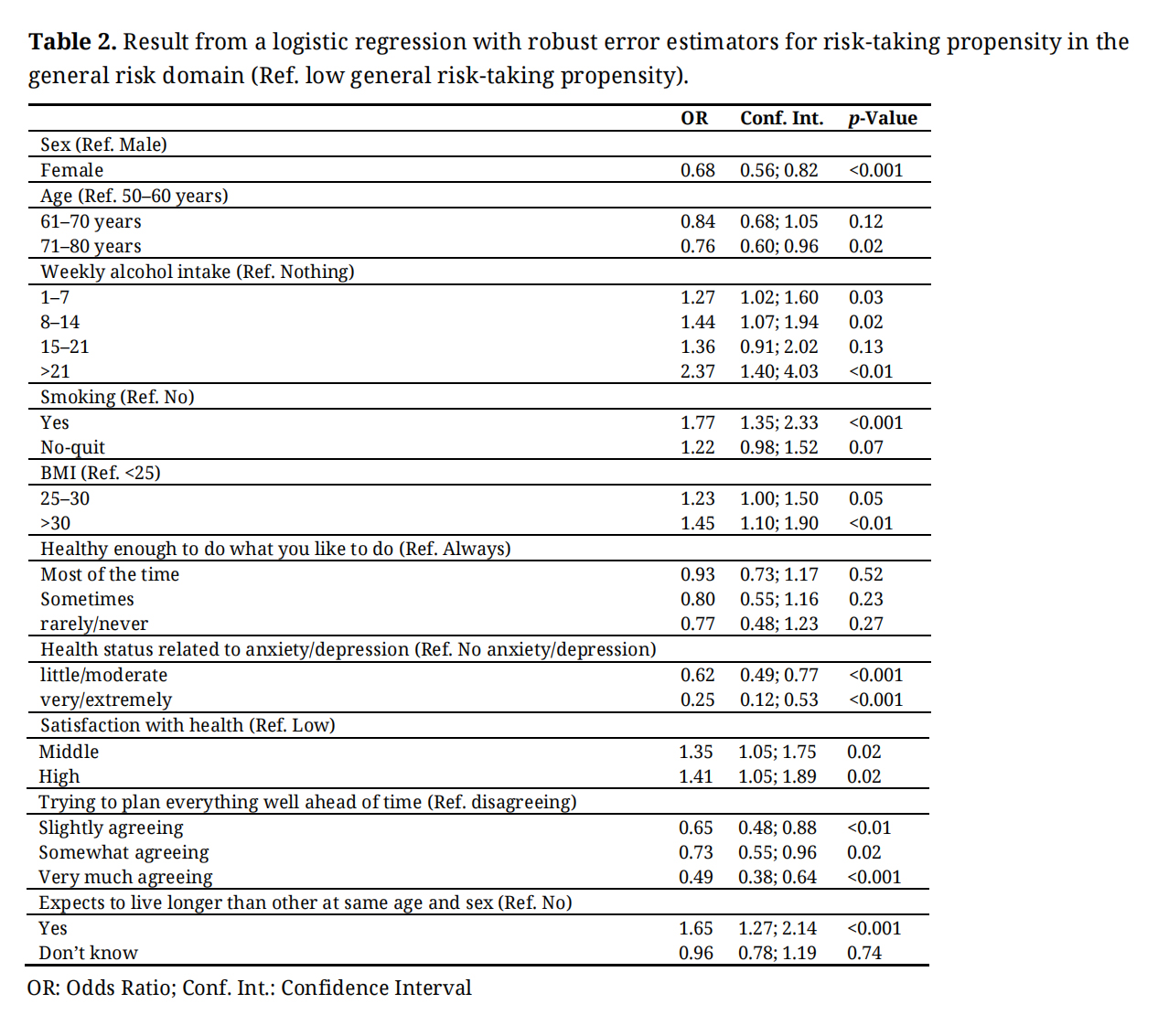 Table 2. Result from a logistic regression with robust error estimators for risk-taking propensity in the general risk domain (Ref. low general risk-taking propensity).
Table 2. Result from a logistic regression with robust error estimators for risk-taking propensity in the general risk domain (Ref. low general risk-taking propensity).
Focusing on the health domain of risk propensity, the regression analysis extracted only but three explanatory variables: having a BMI > 25, smoking, and having a weekly alcohol intake of >21 drinks, whereas the other significant variables from the analysis of general risk propensity no longer appeared significant in the focused regression model (Table 3).
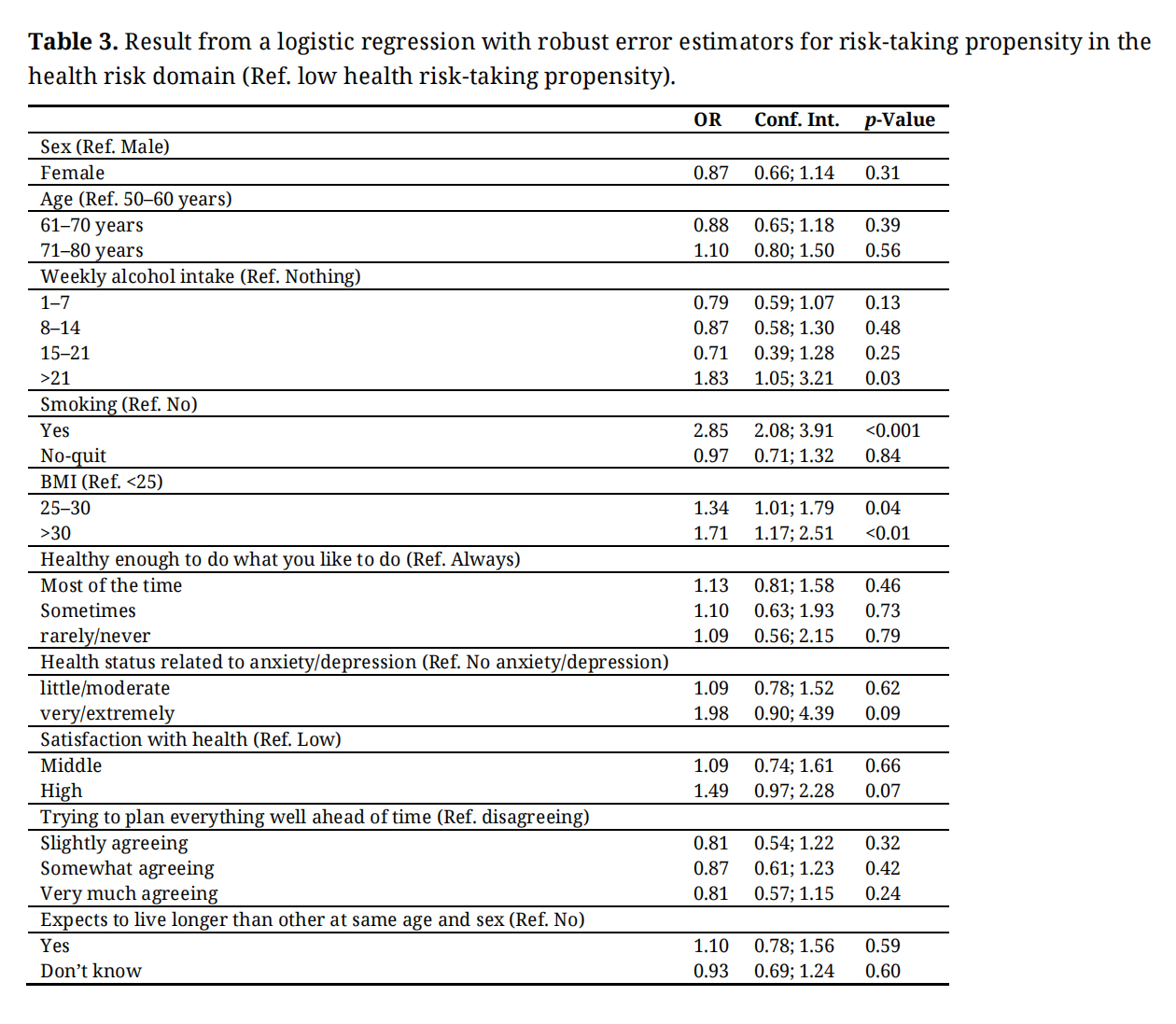 Table 3. Result from a logistic regression with robust error estimators for risk-taking propensity in the health risk domain (Ref. low health risk-taking propensity).
Table 3. Result from a logistic regression with robust error estimators for risk-taking propensity in the health risk domain (Ref. low health risk-taking propensity).
Correlation analyses demonstrated a moderate positive correlation (0.40) between risk propensity within the general and within the health risk domain (Table 4). Also, moderate positive correlations (0.37 and 0.39) were observed between health status related to anxiety/depression and being healthy enough to do what you like and satisfaction with your own health, respectively (Table 4). A strong positive correlation (0.58) was observed between satisfaction with one’s own health and being healthy enough to do what one likes (Table 4).
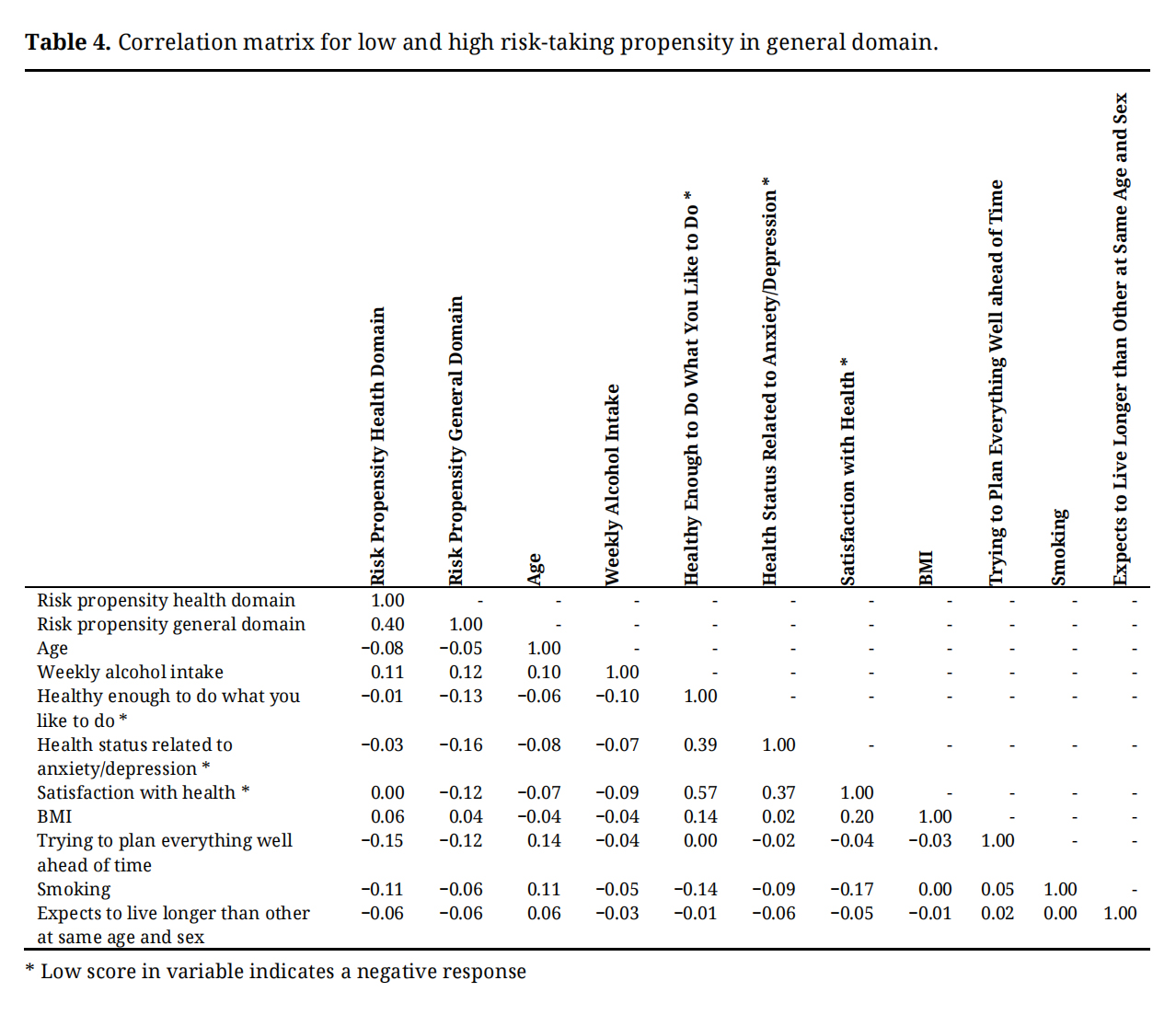 Table 4. Correlation matrix for low and high risk-taking propensity in general domain.
Table 4. Correlation matrix for low and high risk-taking propensity in general domain.
Our study demonstrates that a significantly higher fraction of respondents reports a high risk-taking propensity when framed in the general risk domain (23%) than in the specific health risk domain (4%). This observation is interesting by pointing to the importance of the framed setting used in this kind of studies, where respondents are 5–6 times more willing to take risks if the setting is unspecific compared to the specific health risk domain. Also, this finding may question studies on choices and preferences within the health arena among older adults if the outcome measure reflects a more generalized risk-taking propensity.
Along the same lines, stated expectations to live longer than age and gender-adjusted peers and having higher satisfaction with own health are both associated with a higher risk-taking propensity among our respondents in the general risk domain indicating a higher willingness to take chances if your health situation includes a positive view of the future. This higher general willingness to take chances if in good health does, however, not include the health risk domain. These findings therefore support the caution against using generalized risk scenarios to represent risk-taking propensity in the health domain.
Our observational findings do not allow causative conclusions on the difference between associations between risk propensity and domains, but a recent meta-analysis describes similar findings and suggests that risk propensity should be seen more as independent of the traditional personality traits [12].
An individual’s willingness to take risks is often measured through a questionnaire [1,13,14]. Such stated propensities can be compared with real-life risk-related decisions to demonstrate validity of the measure [3,5,15]. The vast majority of people know that smoking, high alcohol consumption, and a high BMI are all risk factors for your health. If a person smokes, drinks a lot, or has a high BMI it could be seen as risk-taking behavior. High alcohol consumption and smoking are therefore often used as such real-life behavioral choices [1,3,5]. Some authors even consider high risk-taking behavior a vulnerability factor for high alcohol use [16]. Likewise, BMI has been linked to impulsivity [17] and in genetic studies associated with risk propensity [18]. The onset of smoking or excessive alcohol use is, however, in most cases initiated long before people reach 50 years-of-age [19,20]. It is also within younger individuals that a significant correlation between risk-taking propensity and alcohol intake and smoking have been observed [15,21]. As it is within the age groups included in the present study (+50 years-of-age) that lifestyle-related diseases due to smoking and excessive alcohol use become more prevalent, a continuing strong link between these factors and risk propensity could be questioned if such risk-taking behaviors change over a life course depending on what life brings to the individual. The present study, however, demonstrates that exactly these three lifestyle-related factors (smoking, alcohol consumption, and BMI) are the only statistically significant variables explaining the risk-taking propensity in both the general and specific health domains among respondents aged over 50 years. Thus, these observations bring support to the previously reported stability over time of risk-taking propensity also in the older age [7,15].
The age of respondents in the present study (50–80 years-of-age) does not allow conclusions related to younger age groups, but the present findings indicate that these older adults are not willing to take chances related to health, which is also supported by our correlation analyses demonstrating that among our respondents age is neither correlated to being healthy enough to do what you like nor to expectations to live longer than peers of similar age and gender. The absence of a correlation with age indicates that risk-taking propensity within the health domain does not change much after age 50.
The positive and expected correlations between risk propensity in the general and the health domains and also between absence of symptoms related to anxiety/depression and self-experienced health status observed in the correlation analyses all gives support to the validity of the findings and supports the ability of our data set to find relevant correlations if existing.
It is a strength that our net sample is very similar to the Danish population, that we have a response rate of 48%, and that our respondents have almost identical age and sex distribution as the net sample [4]. Furthermore, it is a strength that we have a large sample size of over 7000 respondents, allowing for relevant subgroup analyses. It is a limitation that we do not know how well the stated propensities align with real world behavior, and it is a limitation that we can present associations and correlations but not causality.
The present data demonstrate that risk-taking propensity is domain-specific and specifically risk propensities within the health domain are different from more general risk propensities. This has implications for extrapolating observations based on general risk domains to the health arena. Further, in our group of respondents above 50 years-of-age the modifiable lifestyle-related variables such as smoking, alcohol intake, and BMI are the only significant determinants of risk-taking propensity within the health domain. This confirms the importance of including these variables also in future studies on risk-taking propensity of older individuals.
The present study is a questionnaire study not involving human biological material. According to the Act on the Biomedical Research Ethics Committee System in Denmark, the project was therefore not a biomedical research project and the need for consent was waived (Danish Act on Research Ethics Review of Health Research Projects; §14 stk. 2, June 2011). Data includes information that could potentially identify individuals, and the project is therefore registered at the University’s Research and Innovation Office, and data handling is in accordance with the General Data Protection Regulation (GDPR) from (EU) 2016/679.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
JBN planned, and was the lead author on the manuscript, and both authors (JBN, HSA) analyzed the data, and read and approved the final manuscript.
The author(s) received no financial support for the research and/or publication of this article.
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
The authors declare no conflicts of interest.
Not applicable.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Nielsen JB, Andersen HS. Associations between risk-taking propensity and individual lifestyle and behavioral characteristics—Analyses on survey data from 7232 Danes aged 51–80 years-of-age. Adv Geriatr Med Res. 2025;7(3):e250019. https://doi.org/10.20900/agmr20250019.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




