Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(2):e260010. https://doi.org/10.20900/agmr20260010
1 Department of Surgery, School of Medicine, Virginia Commonwealth University, Medical Center West Hospital, Room B 048, 1200 E Broad Street, Richmond, VA 23219, USA
2 Department of Psychiatry School of Medicine, Virginia Commonwealth University, Richmond, VA 23284, USA
3 Department of Gerontology College of Health Professions, Virginia Commonwealth University, Richmond, VA 23284, USA
* Correspondence: Asmaa Namoos
Introduction: Falls are a major source of morbidity in older adults and pose particular concern in cancer survivors who may experience treatment related neurological and functional decline. Dementia is a known risk factor for falls, yet its contribution to fall risk among breast cancer survivors has not been well defined. Methods: This retrospective cohort study used de identified electronic health records from the TriNetX Research Network, which includes more than 100 health care organizations. Women aged 65 years or older with stage 1 to stage 3 breast cancer were eligible. Dementia was identified using ICD 10 code F03 recorded on or after the first qualifying cancer diagnosis. Propensity score matching used a 1 to 1 nearest neighbor approach. The primary outcome was incident fall events identified by ICD 10 codes for unspecified falls, initial fall encounters, history of falling, and repeated falls. Multivariable Cox proportional hazards models estimated independent predictors of falls. Follow up began 1 day after diagnosis and continued through the last recorded encounter. Results: A total of 49,576 breast cancer survivors met inclusion criteria, of whom 1683 (3.4%) had dementia. Before matching, fall related diagnoses were significantly more common in patients with dementia, including unspecified falls (26% vs. 2%, p < 0.0001) and history of falling (15% vs. 1%, p < 0.0001). After 1 to 1 matching, 1 602 survivors remained in each cohort with standardized mean differences < 0.06 across all variables. During follow up, 17.8% of survivors with dementia experienced a fall compared with 6.5% without dementia. This corresponded to an absolute risk difference of 11.3% (95% CI 9.1% to 13.6%), a risk ratio of 2.74 (95% CI 2.41 to 3.12), and an odds ratio of 3.12 (95% CI 2.67 to 3.65). The Kaplan Meier analysis showed significantly lower fall free survival in the dementia cohort (log rank p < 0.0001). The adjusted Cox model showed that dementia remained an independent predictor of falls (hazard ratio 1.43, 95% CI 1.25 to 1.63). Additional strong predictors included long term drug therapy (hazard ratio 2.62, 95% CI 2.41 to 2.84), osteoporosis (hazard ratio 1.48, 95% CI 1.34 to 1.62), polyneuropathy (hazard ratio 1.58, 95% CI 1.34 to 1.85), and depressive episode (hazard ratio 1.78, 95% CI 1.60 to 1.98). Conclusions and Relevance: Dementia was associated with a substantially elevated fall risk among older breast cancer survivors, even after extensive adjustment for comorbidity, neurological conditions, psychiatric disorders, and medication burden. Recognition of this risk may help clinicians identify a subgroup of survivors who require closer monitoring and more precise evaluation during routine care.
Recent research in cancer neuroscience is reshaping our understanding of how tumors and the brain communicate. Cancer is not confined to unchecked cell growth; it interacts with neural circuits and the central nervous system in ways that influence tumor progression, repair, inflammation, and even systemic vulnerability. In parallel, the burdens of cancer treatment often extend beyond the tumor management; treatments affect brain health, cognition, neurological resilience, and physical function [1,2]. In survivors of breast cancer, this “neural legacy” can manifest as subtle to overt cognitive dysfunction, neuropathy, and neurologic comorbidities.
Many breast cancer survivors report persistent cognitive changes such as slower information processing, difficulties with attention or multitasking, and memory lapses [3,4]. This phenomenon, often termed cancer-related cognitive impairment (CRCI), has been documented across many studies, even years after treatment ends [5]. In survivors, factors such as surgical stress, chemotherapy, radiation, endocrine therapy, brain aging, and systemic inflammation may act in concert to weaken neural reserve and plasticity [6]. Moreover, these cognitive changes do not occur in isolation: they often overlap with other treatment sequelae such as peripheral neuropathy, fatigue, sarcopenia, and functional decline [7]. Beyond these treatment related effects, breast cancer survivorship itself may heighten vulnerability to falls through interacting neurologic, musculoskeletal, and functional pathways. Peripheral neuropathy, sarcopenia, fatigue, balance impairment, and treatment associated frailty may collectively compromise mobility and postural stability. Cognitive impairment may further amplify these vulnerabilities through impaired attention, executive dysfunction, and reduced ability to adapt to environmental hazards, providing a biologically and clinically plausible link among breast cancer, dementia, and elevated fall risk.
In older adults, cognitive vulnerability is a known contributor to fall risk [8,9]. Impaired attention, slowed reaction time, reduced capacity to adapt to environmental challenges, and poorer executive control all compromise physical balance and increase the likelihood of missteps or instability [10]. Among patients with dementia or mild cognitive impairment, fall rates are significantly higher compared to peers with normal cognitive function [11]. Yet, little is known about how this risk plays out in the context of cancer survivorship, where multiple intersecting vulnerabilities (e.g., older age, prior treatments, comorbid disease, polypharmacy) coexist. Race and ethnicity were also considered relevant to this framework given documented disparities in fall risk, comorbidity burden, functional decline, and survivorship outcomes among older adults with cancer.
Breast cancer survivors represent a particularly important population in this regard. Because breast cancer is common and survival rates are high, a growing number of women live long after diagnosis and therapy [12]. As this survivor population ages, neurological and functional health become central to quality of life and independence. However, in this group, the interplay between preexisting or new-onset dementia and fall risk remains largely unexplored. Anecdotally, clinicians observe that older survivors with cognitive impairment may fall more, but published evidence is scarce [7].
Our study seeks to fill this gap by quantifying the comparative risk of falls among older breast cancer survivors with versus without dementia, using a large real-world electronic health record network. We also aim to disentangle the independent effect of dementia after adjusting for demographic, frailty, neurologic and psychiatric comorbidities, and medication burden. We hypothesize that dementia will remain a robust independent predictor of fall risk, even in this medically complex population. By doing so, we hope to inform fall-prevention strategies tailored for cognitively impaired cancer survivors and guide risk stratification in survivorship care.
Data Source. This retrospective cohort study utilized data from the TriNetX Research Network, a federated platform aggregating de-identified electronic health records from more than 100 health care organizations. TriNetX enables the construction of complex cohort queries based on diagnosis, procedure, demographic, and temporal parameters while maintaining full compliance with HIPAA and GDPR standards. All data are de-identified prior to analysis; therefore, institutional review board approval was not required.
Study Population. Cohorts were identified using ICD-10-CM code C50 (malignant neoplasm of breast) and AJCC stage information from the TriNetX Research Network [13]. Eligible participants were women aged 65 years or older with stage I–III breast cancer and complete follow-up data. Stage 0 cases were excluded because in situ disease rarely leads to treatment-related cognitive or physical decline, while stage IV cases were excluded due to advanced illness and high baseline fall risk. Limiting the sample to stages I–III ensured a comparable survivorship population for evaluating dementia-related fall risk. After applying these criteria, 1684 dementia cases and 55,837 non-dementia comparators were retained for baseline analyses. Minor differences between the initial and analytic counts reflect automated TriNetX data-quality filters, which exclude records with missing variables or inconsistent temporal relationships between diagnoses, such as dementia documented before the breast cancer diagnosis. At the time of analysis, data were contributed by 109 of 111 participating health care organizations across the network (Figure 1).
Time Window and Index Event. A five-year look-back period (1825 days) was applied to ensure accurate temporal alignment between dementia and breast cancer diagnoses. The index date was defined as the first recorded breast cancer diagnosis meeting all inclusion criteria. The observation window extended from 1825 days before to 1 day prior to the index event, ensuring that dementia or comparator diagnoses occurred within a clinically relevant period while excluding cases in which dementia pre-dated the cancer diagnosis.
Dementia Cohort Definition. The dementia cohort included women aged 65 years and older with a documented diagnosis of unspecified dementia (ICD-10-CM F03) recorded on or after the index breast cancer diagnosis. ICD 10 code F03 for unspecified dementia was selected to maximize capture of clinically documented dementia across participating health systems within the TriNetX network, recognizing variability in subtype specific coding across institutions. This specification allowed same-day documentation but excluded any dementia diagnosis occurring before cancer diagnosis to capture cognitive decline concurrent with or following breast cancer. The comparison cohort comprised patients who met all other eligibility criteria but had no record of dementia (F03) during the observation period. Dementia was modeled as a baseline exposure rather than a time varying covariate and was operationalized as a documented diagnosis occurring on or after breast cancer diagnosis and before follow up for incident falls. This temporal structure was intended to ensure that dementia status preceded or coincided with the fall risk observation period.
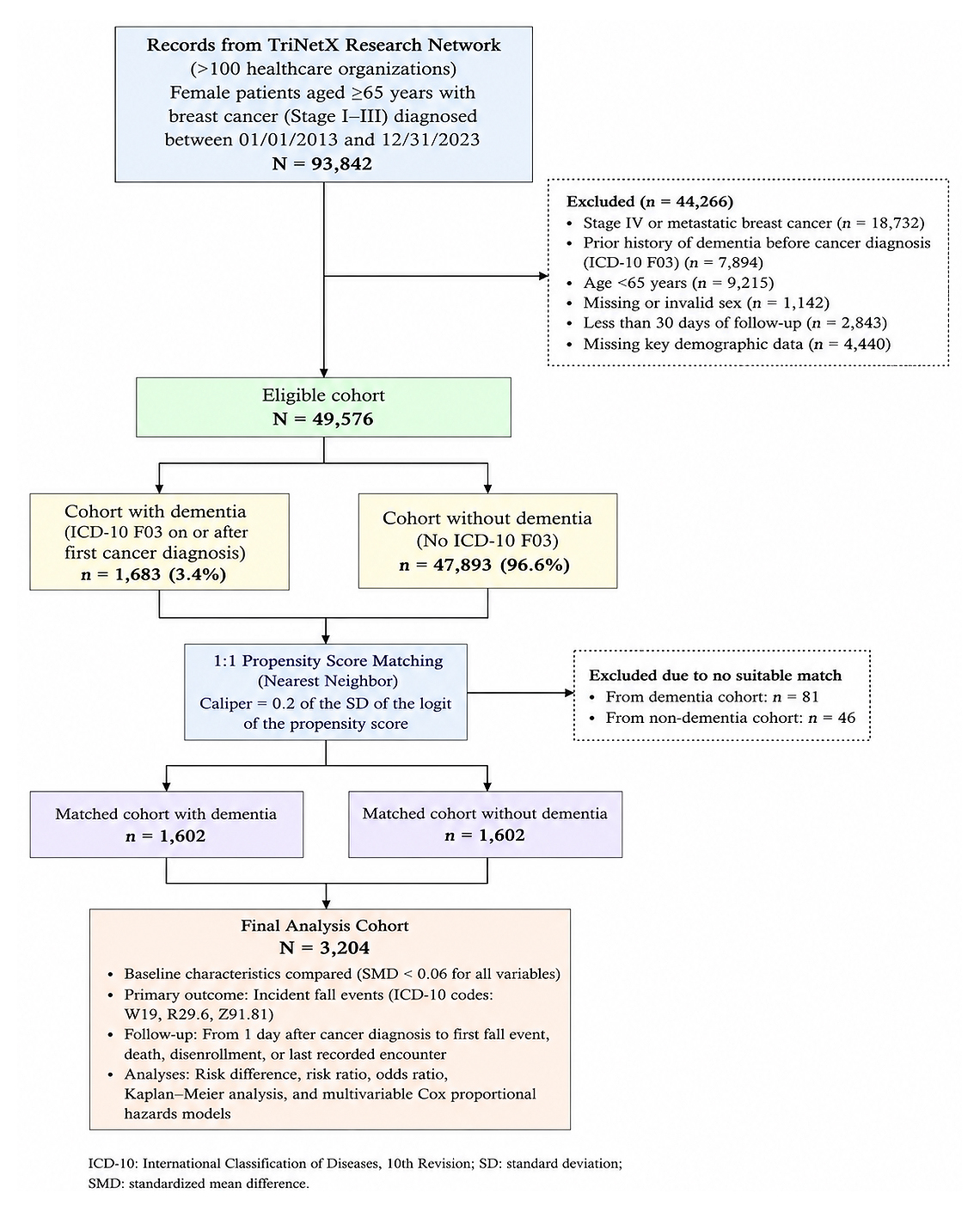 Figure 1. Study Flowchart.
Figure 1. Study Flowchart.
Outcome Definition. The primary outcome was the occurrence of a fall following the breast cancer diagnosis. Fall-related events were defined using ICD-10-CM codes W19 (unspecified fall), W19.XXXA (unspecified fall, initial encounter), Z91.81 (history of falling), and R29.6 (repeated falls). To ensure that only incident falls were captured, patients with documented fall diagnoses prior to the index breast cancer diagnosis were excluded. The index date was defined as the earliest recorded date of breast cancer diagnosis. Patients were followed from one day after the index date until the last available encounter, death, or censoring. Patients were followed from 1 day after the index date until first fall event, death, loss to follow up, or censoring at the last recorded encounter. Time to event analyses evaluated timing from breast cancer diagnosis to first documented fall. The composite fall outcome captured both single fall events and recurrent falls, including repeated falls identified through ICD 10 code R29.6. Recurrent falls were included within the primary outcome definition, although they were not modeled as a separate outcome in the primary analysis.
Covariates. Clinical covariates were selected based on prior literature, clinical relevance, and documented disparities in fall risk and survivorship outcomes. These included demographic factors (age, race, and ethnicity), frailty and musculoskeletal conditions (osteoporosis, sarcopenia, cachexia, muscle wasting), neurological disorders (polyneuropathy, Parkinson’s disease, sequelae of cerebral infarction, unsteadiness, and other gait abnormalities), psychiatric conditions (major depressive disorder and depressive episodes), comorbidities (heart failure, malnutrition, pressure ulcer), and medication burden, represented by long-term drug therapy (ICD-10-CM Z79) as a proxy for polypharmacy (Table 1).
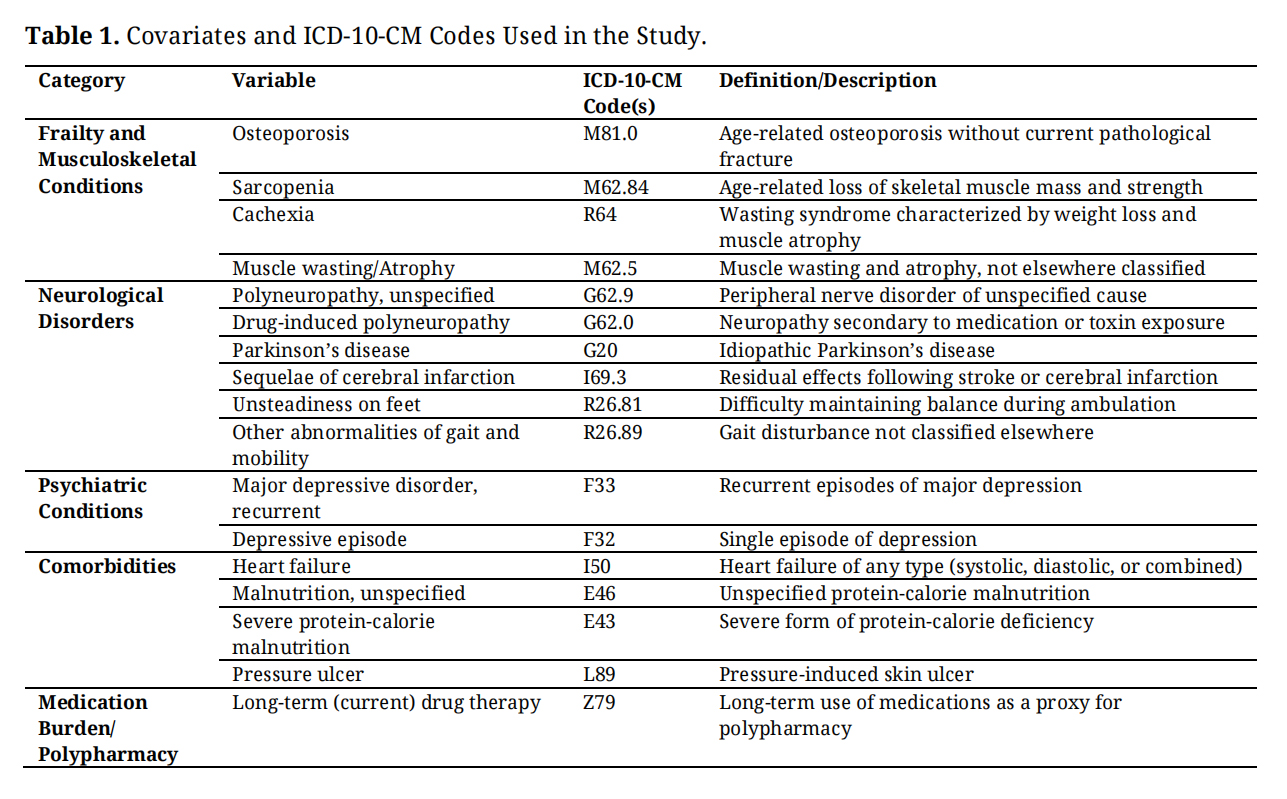 Table 1. Covariates and ICD-10-CM Codes Used in the Study.
Table 1. Covariates and ICD-10-CM Codes Used in the Study.
Statistical Analysis. Descriptive statistics were used to summarize baseline characteristics of the dementia and non-dementia cohorts. Continuous variables were compared using Student’s t tests, and categorical variables were compared using chi square tests. Standardized mean differences were calculated to assess covariate balance, with values below 0.1 indicating adequate balance. To reduce confounding, 1 to 1 nearest neighbor propensity score matching was performed, and covariate balance was reassessed after matching. Kaplan Meier curves were generated to compare fall free survival between cohorts, and differences were evaluated using the log rank test.
Age was treated as a key potential confounder given its strong association with both dementia and fall risk. Accordingly, age and age at breast cancer diagnosis were incorporated into the propensity score model, resulting in near identical age distributions between cohorts after matching, with standardized mean differences below 0.06. Following matching, Cox proportional hazards regression models were fitted to estimate the independent association between dementia and risk of falling. Dementia exposure was treated as fixed at baseline and was not modeled as a time varying covariate. Age at index diagnosis was additionally included in the multivariable model as a conservative residual adjustment alongside race, comorbidities, frailty, neurologic and psychiatric conditions, and polypharmacy. Hazard ratios with 95% confidence intervals were reported, and statistical significance was defined as a two-sided p value < 0.05. All analyses were conducted within the TriNetX analytics environment using its built-in statistical functions. Model assumptions were evaluated within the TriNetX analytics environment, including assessment of proportional hazards assumptions for Cox models. Covariate selection was guided to minimize multicollinearity and preserve model stability, and model specification was reviewed for plausibility.
Baseline Demographics. Breast cancer survivors with dementia (n = 1683) differed substantially from those without dementia (n = 48,926) in demographic composition and fall-related health profiles (Table 2). All participants were female and aged 65 years or older. The dementia cohort was significantly older, with a mean current age of 84.3 ± 6.44 years compared with 76.3 ± 7.54 years among survivors without dementia (p < 0.0001). The mean age at index cancer diagnosis was also higher in the dementia group (79.9 ± 7.40 years) than in the non-dementia group (67.2 ± 8.84 years; p < 0.0001). Racial and ethnic distributions varied significantly. Survivors with dementia were more frequently White (66%) or Black/African American (25%) than those without dementia (59% and 11%, respectively; both p < 0.0001). In contrast, the non-dementia cohort included a greater proportion of patients with Unknown race (18% vs. 2%) and the other race (6% vs. 2%). Rates of Asian, Hispanic/Latino, and Native Hawaiian/Pacific Islander categories were low and did not differ significantly. In contrast, American Indian/Alaska Native representation, although small in absolute numbers, differed significantly between cohorts. Similarly, more dementia patients were identified as Not Hispanic or Latino (70% vs. 50%, p < 0.0001), whereas Unknown ethnicity was more common in the non-dementia group (46% vs. 27%, p < 0.0001). These findings indicated significant baseline heterogeneity between the two cohorts prior to adjustment (Table 2).
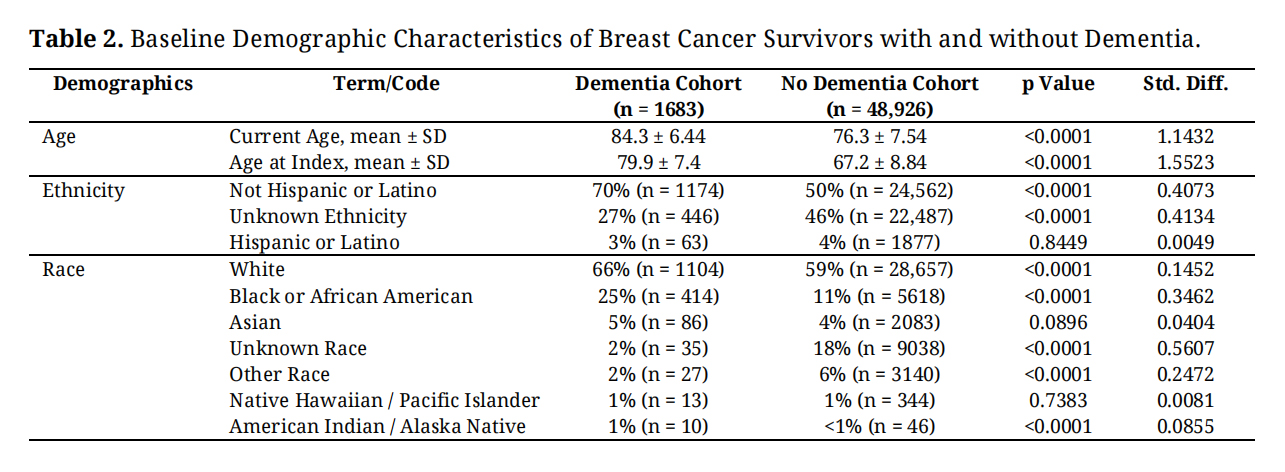 Table 2. Baseline Demographic Characteristics of Breast Cancer Survivors with and without Dementia.
Table 2. Baseline Demographic Characteristics of Breast Cancer Survivors with and without Dementia.
Baseline Fall-Related Diagnoses. Before the index breast cancer diagnosis, fall-related conditions were more frequently documented among survivors with dementia than among those without dementia. Unspecified falls were recorded in 26% (n = 434) of the dementia cohort and in 2% (n = 1038) of the non-dementia cohort (p < 0.0001; standardized difference 0.73). Initial encounters for unspecified falls occurred in 25% (n = 415) of survivors with dementia and in 2% (n = 980) of those without dementia (p < 0.0001; standardized difference 0.71). The history of falling was present in 15% (n = 259) of the dementia cohort and in 1% (n = 403) of the non-dementia cohort (p < 0.0001; standardized difference 0.55). Repeated falls were recorded in 11% (n = 180) of survivors with dementia compared with less than 1% (n = 191) of those without dementia (p < 0.0001; standardized difference 0.46). Fall-related injuries coded as injury of unspecified body region (T14) were reported in 8% (n = 141) of the dementia cohort and in 1% (n = 576) of the non-dementia cohort (p < 0.0001; standardized difference 0.34) (Table 3).
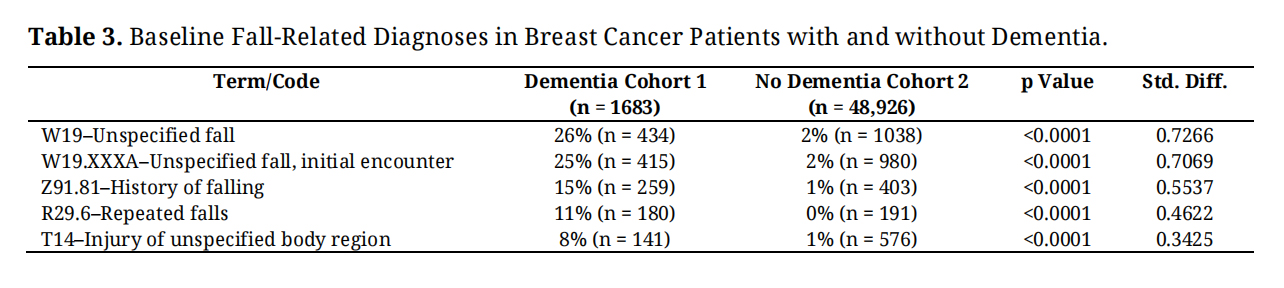 Table 3. Baseline Fall-Related Diagnoses in Breast Cancer Patients with and without Dementia.
Table 3. Baseline Fall-Related Diagnoses in Breast Cancer Patients with and without Dementia.
After 1:1 propensity score matching, 1602 patients were retained in each cohort. Matching achieved excellent balance across all demographic covariates, with standardized mean differences below 0.06 (Table 3). Mean current age was virtually identical between dementia and non-dementia patients (84.1 ± 6.50 vs. 84.1 ± 6.56 years, p = 0.98), as was age at index diagnosis (79.5 ± 7.39 vs. 79.5 ± 7.52 years, p = 0.99). Racial and ethnic distributions were similarly well balanced after matching. The proportion of White (65.6% vs. 65.4%) and Black/African American (24.3% vs. 25.5%) patients was nearly identical, and no residual significant differences remained across Asian, Hispanic/Latino, or other racial categories (all p > 0.05). Ethnic proportions also aligned closely (Not Hispanic or Latino 69.7% vs. 72.0%; p = 0.15) (Table 4). After matching, mean age at breast cancer diagnosis and current age were identical between cohorts, indicating excellent control of age-related confounding.
Baseline Fall-Related Diagnoses. Prior to propensity score matching, fall-related conditions were markedly more prevalent among breast cancer survivors with dementia compared to those without. Unspecified falls (W19) were documented in 25.8% of the dementia cohort versus 2.1% of the non-dementia cohort (p < 0.0001). Similarly, initial encounters for unspecified falls (W19) occurred in 24.7% versus 2.0% of patients, respectively (p < 0.0001). A documented history of falling (Z91.81) was present in 15.4% of dementia patients compared with 0.8% of those without dementia (p < 0.0001). Repeated falls (R29.6) were identified in 10.7% versus 0.4% (p < 0.0001), and injuries of unspecified body region (T14) were more frequent among dementia patients (8.4% vs. 1.2%; p < 0.0001).
After 1:1 propensity score matching (Figure 2), these conditions were well balanced across groups. The matched dementia and non-dementia cohorts each included 1,602 patients, with nearly identical frequencies of unspecified falls (22.9% vs. 23.1%; p = 0.87), initial encounters for unspecified falls (21.8% vs. 22.2%; p = 0.77), history of falling (12.6% vs. 11.2%; p = 0.25), repeated falls (8.4% vs. 7.0%; p = 0.14), and injury of unspecified body region (7.4% vs. 7.9%; p = 0.60). All standardized mean differences were below 0.06, confirming adequate balance in fall-related diagnoses following matching (Table 5).
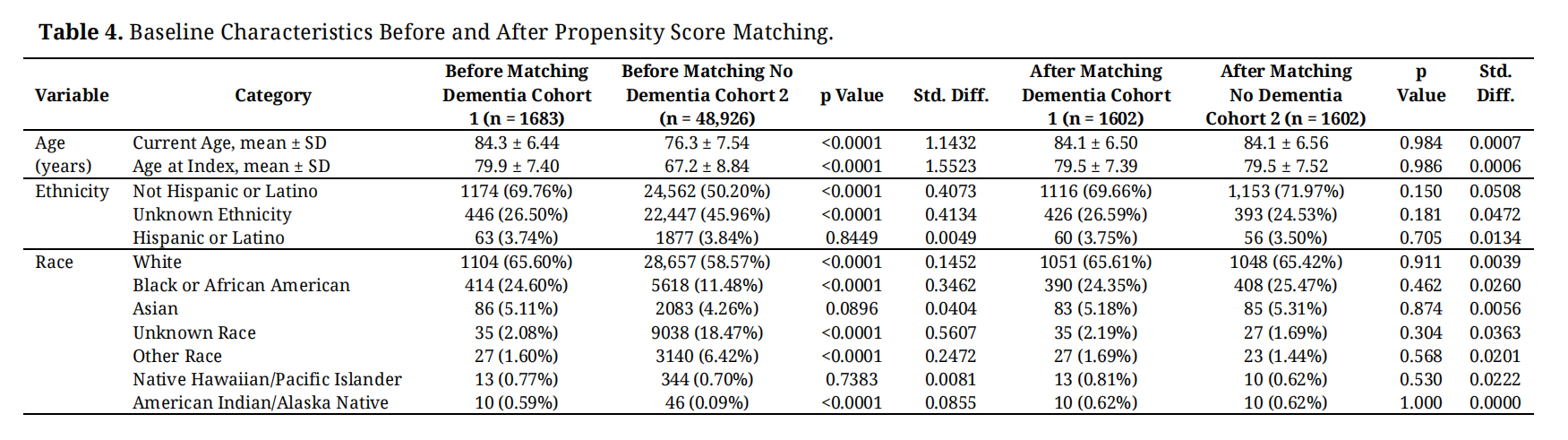 Table 4. Baseline Characteristics Before and After Propensity Score Matching.
Table 4. Baseline Characteristics Before and After Propensity Score Matching.
 Table 5. Baseline Fall-Related Diagnoses Before and After Propensity Score Matching.
Table 5. Baseline Fall-Related Diagnoses Before and After Propensity Score Matching.
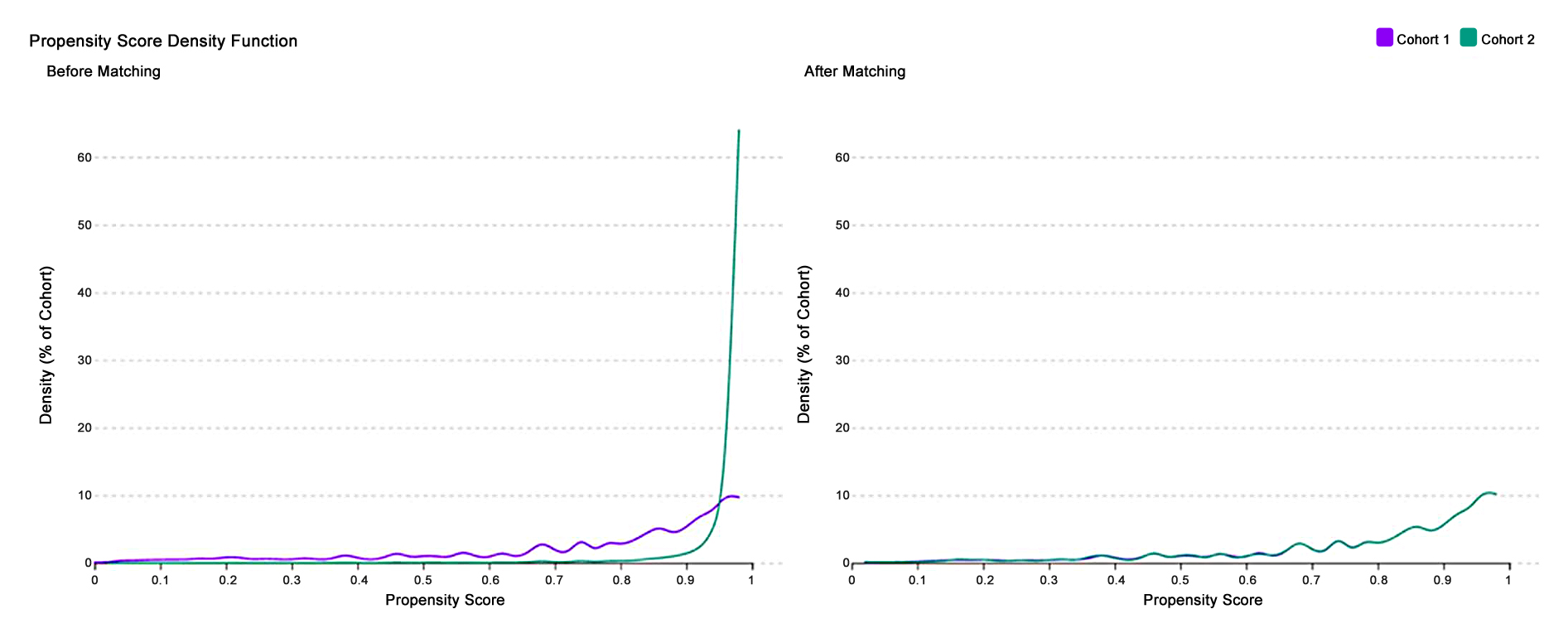 Figure 2. Propensity score distributions before and after matching.
Figure 2. Propensity score distributions before and after matching.
Measures of Association. After excluding patients with falls prior to the index period (cancer diagnosis), breast cancer survivors with dementia exhibited a significantly higher risk of subsequent falls compared with those without dementia. Among the dementia cohort, 17.8% (202 of 1,134) experienced a fall during follow-up compared with 6.5% (3,096 of 47,639) in the non-dementia cohort. The absolute risk difference was 11.3% (95% CI 9.1–13.6, p < 0.0001), while the relative risk was 2.74 (95% CI 2.41–3.12). Similarly, the odds of falling were more than three times higher in the dementia group compared to the non-dementia group (odds ratio 3.12, 95% CI 2.67–3.65) (Table 6).
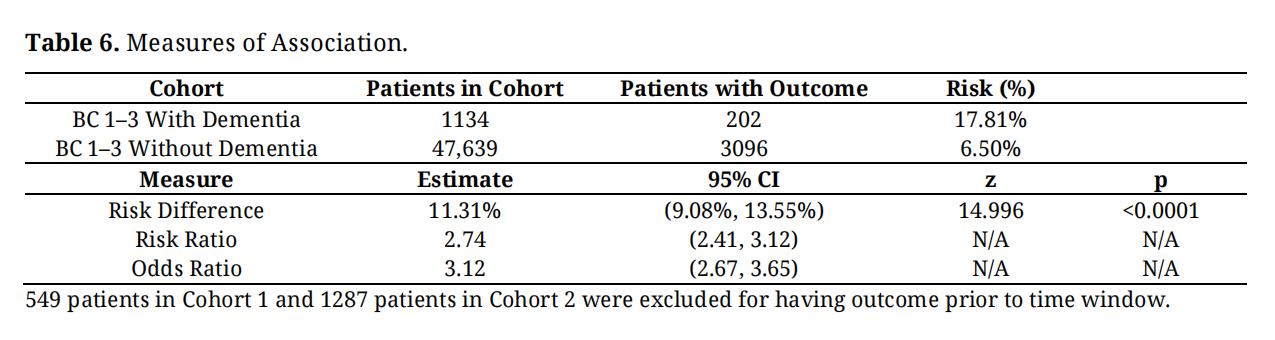 Table 6. Measures of Association.
Table 6. Measures of Association.
Kaplan–Meier Survival Analysis. Survival analysis (Figure 2) further highlighted the heightened fall risk in patients with dementia. The median survival time to first fall in the dementia cohort was 4,161 days, with only 47.6% of patients remaining fall-free at the end of the follow-up window, compared with 78.9% in the non-dementia cohort. Reporting median time to first fall provides additional context for the temporal relationship between breast cancer diagnosis and fall occurrence beyond relative risk estimates. The log-rank test revealed a highly significant difference between survival curves (χ² = 876.3, df = 1, p < 0.0001). The hazard of falling was more than six times higher among breast cancer survivors with dementia (HR = 6.57, 95% CI 5.69–7.59, p = 0.0008) (Figure 3).
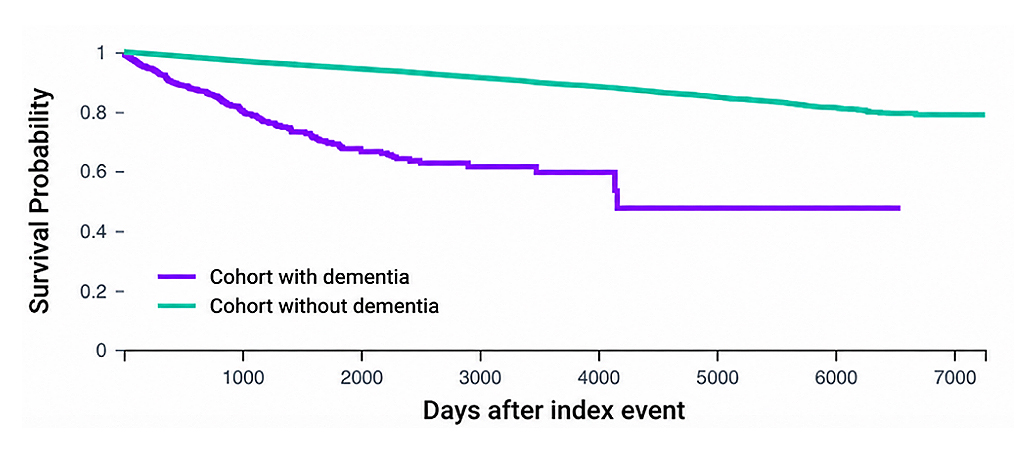 Figure 3. Kaplan Meier Survival Curve by Dementia Status.
Figure 3. Kaplan Meier Survival Curve by Dementia Status.
Number of Fall Instances. When the frequency of fall episodes was evaluated, dementia patients averaged slightly more fall events than those without dementia (2.44 ± 8.20 vs. 2.04 ± 5.05). However, this difference was not statistically significant (t = 1.05, df = 3296, p = 0.29). Median fall count was one in both cohorts, suggesting that while dementia substantially increases the likelihood and timing of falls, the total number of fall episodes per patient among those who do fall does not differ meaningfully by dementia status. Although recurrent falls were therefore partially examined descriptively, the primary analysis focused on overall fall occurrence rather than modeling recurrent falls as a distinct endpoint. Future studies should examine whether dementia differentially influences risk of repeated versus isolated falls
Cox Proportional Hazards AnalysisA multivariable Cox proportional hazards model was used to examine predictors of fall-related outcomes among older breast cancer survivors. Dementia status was independently associated with a significantly higher hazard of falls (HR = 1.43, 95% CI: 1.25–1.63, p < 0.001) after adjustment for demographic, clinical, and functional covariates (Table 7).
Age and Demographics. Each one-year increase in age at index was associated with a 5.4% increase in fall risk (HR = 1.05, 95% CI: 1.05–1.06, p < 0.001). Race and ethnicity were significant predictors: Black or African American patients had a 30% higher hazard of falls compared with White patients (HR = 1.31, 95% CI: 1.20–1.42, p < 0.001), while Hispanic or Latino patients had the highest relative risk (HR = 1.77, 95% CI: 1.55–2.03, p < 0.0001).
Frailty and Musculoskeletal Conditions. Among frailty-related variables, osteoporosis (HR = 1.48, 95% CI: 1.34–1.62, p < 0.001) and cachexia (HR = 2.44, 95% CI: 1.45–4.08, p = 0.001) were strong independent predictors of falls. Sarcopenia and muscle wasting were not statistically significant (p = 0.44 and p = 0.71, respectively).
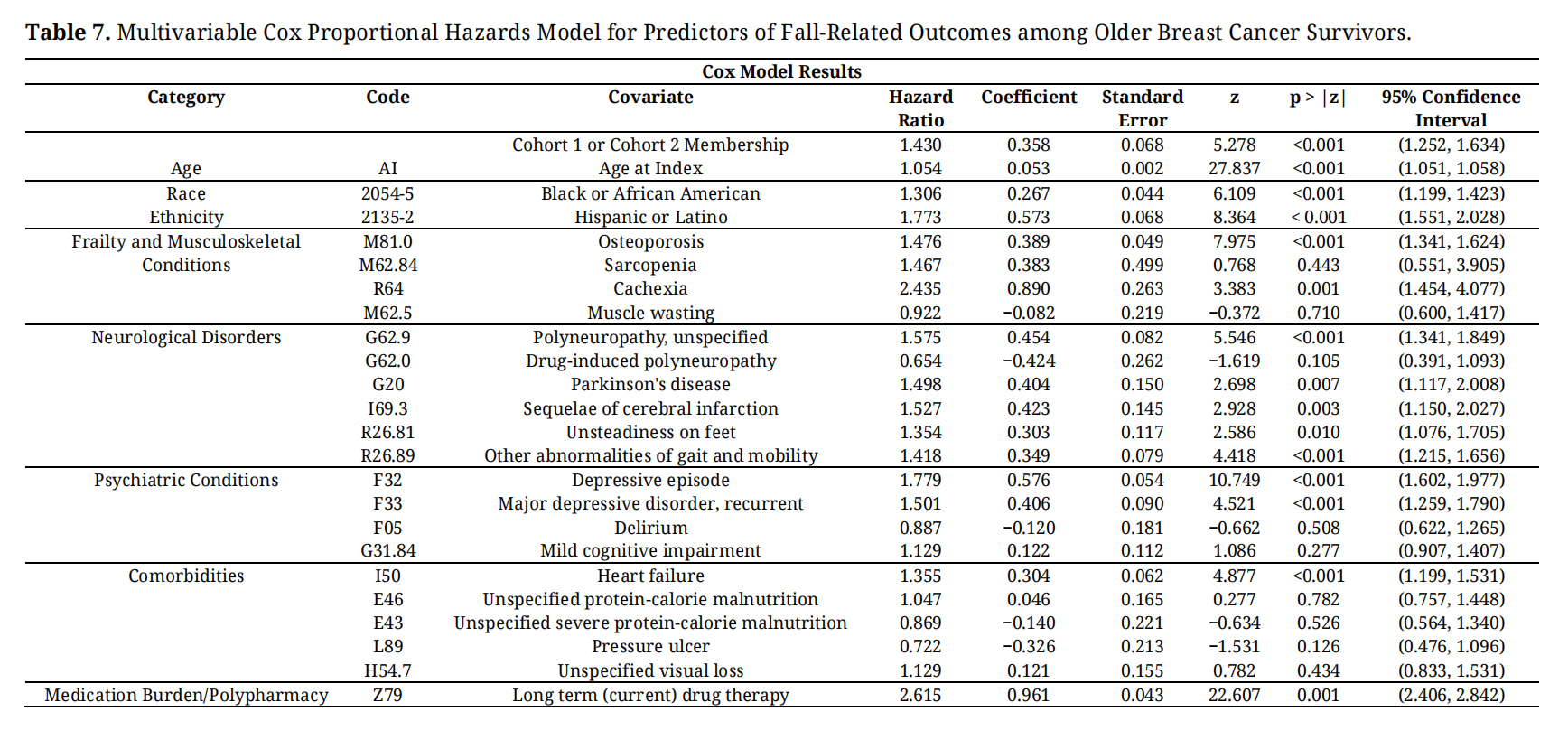 Table 7. Multivariable Cox Proportional Hazards Model for Predictors of Fall-Related Outcomes among Older Breast Cancer Survivors.
Table 7. Multivariable Cox Proportional Hazards Model for Predictors of Fall-Related Outcomes among Older Breast Cancer Survivors.
Neurological Disorders. Polyneuropathy was associated with a 57% higher hazard of falls (HR = 1.58, 95% CI: 1.34–1.85, p < 0.001), while Parkinson’s disease (HR = 1.50, 95% CI: 1.12–2.01, p = 0.007) and sequelae of cerebral infarction (HR = 1.53, 95% CI: 1.15–2.03, p = 0.003) were also significant. Unsteadiness on feet (HR = 1.35, 95% CI: 1.08–1.71, p = 0.010) and other gait abnormalities (HR = 1.42, 95% CI: 1.22–1.66, p < 0.001) further contributed to elevated fall risk.
Psychiatric Conditions. Both depressive episodes (HR = 1.78, 95% CI: 1.60–1.98, p < 0.001) and recurrent major depressive disorder (HR = 1.50, 95% CI: 1.26–1.79, p < 0.001) were independently associated with increased fall risk. Delirium and mild cognitive impairment were not significant predictors (p = 0.51 and p = 0.28, respectively).
Comorbidities. Heart failure was a significant predictor of falls (HR = 1.36, 95% CI: 1.20–1.53, p < 0.001), whereas malnutrition, pressure ulcers, and visual loss did not reach statistical significance (all p > 0.12).
Medication Burden. Long-term drug therapy, used as a proxy for polypharmacy (ICD-10-CM Z79), was among the strongest predictors, associated with more than a twofold increased hazard of falls (HR = 2.62, 95% CI: 2.41–2.84, p < 0.001).
Because age was balanced through matching and further adjusted in the multivariable model, the association between dementia and fall risk is unlikely to be explained by residual age confounding.
This large real- world cohort study provides new insights into the relationship between dementia and fall risk among older breast cancer survivors. We observed that survivors with dementia were more than twice as likely to experience a fall compared with survivors without dementia, and this increased risk persisted after controlling for a comprehensive set of demographics, clinical and treatment -related factors. The absolute risk difference of 11.3 percentage points translates into a substantial burden of fall-related events in this population. These findings align with broader geriatric literature showing that cognitive impairment markedly increases the likelihood of falls: older adults with dementia fall two to three times more often than cognitively healthy peers, and between 60-80% of people with dementia fall annually [11]. Our results extend these observations by showing that dementia remains an independent predictor of falls even after accounting for frailty, neurological disorders, psychiatric conditions and polypharmacy, suggesting a distinctive vulnerability among cognitively impaired cancer survivors. Importantly, this study contributes new knowledge by being among the first large multicenter real-world analyses to evaluate dementia as an independent fall risk factor specifically in older breast cancer survivors. By integrating oncology survivorship, cognitive vulnerability, and fall outcomes within a single analytic framework, this work extends existing geriatric and oncology literature and supports incorporation of cognitive status into fall risk stratification and survivorship planning.
Several covariates emerged as important contributors to fall risk. Increasing age at cancer diagnosis was associated with a higher hazard of falling, consistent with evidence that falls affect more than thirty percent of adults aged sixty-five years and older [14]. Race and ethnicity were also significant predictors: Black and Hispanic survivors faced greater hazards compared with White survivors [15]. Frailty -related conditions such as osteoporosis and cachexia, neurologic disorders including polyneuropathy, Parkinson disease and sequelae of cerebral infarction, and psychiatric disorders such as depressive episodes all conferred elevated fall risk [16–19]. Notably, long -term use of medications a proxy for polypharmacy was one of the strongest predictors, more than doubling the hazard of falling [20]. These findings highlight the multifactorial nature of falls, which are influenced by interactions between neuromuscular function, cognition, comorbidity burden, medication effects and sociodemographic factors. They also underscore the importance of comprehensive geriatric assessment in oncology practice, with attention to medication management and mental health.
Our findings have several implications for clinical care and survivorship planning. First, they emphasize the need for proactive fall- prevention strategies tailored to older breast cancer survivors with dementia. Interventions such as balance and strength training, home safety assessments, medication review and cognitive support should be integrated into survivorship care plans. Second, the strong association between polypharmacy and falls supports efforts to deprescribe non- essential medications and to coordinate care across oncology, primary care and geriatrics. Third, the elevated risk among Black and Hispanic survivors signals potential disparities in access to supportive services or differences in comorbidity profiles; culturally informed interventions and equitable access to fall- prevention programs are needed. Finally, because older adults with dementia fall frequently, clinicians should consider routine cognitive screening for breast cancer survivors and engage caregivers in fall- prevention education. Future research should examine the efficacy of multifaceted interventions in this population, explore mechanisms linking cognitive impairment and falls, and investigate how cancer treatments interact with dementia- related neuropathology to influence mobility and balance.
An additional consideration is the potential bidirectional relationship between falls and cognitive decline. While dementia may increase susceptibility to falls through impaired executive function, gait instability, and reduced attentional control, recurrent falls may also reflect or contribute to worsening cognition through injury, reduced mobility, fear of falling, and diminished physical and social engagement. Thus, falls may function not only as an outcome of cognitive vulnerability but also as a possible marker of progressive decline. Future longitudinal studies are needed to better characterize these reciprocal pathways among older breast cancer survivors.
Age is a dominant risk factor for both dementia and falls. In this study, age differences between cohorts were addressed primarily through propensity score matching, which achieved nearly identical age distributions between dementia and non-dementia survivors. The persistence of the dementia association after matching and multivariable adjustment suggests that dementia confers excess fall risk beyond chronological aging alone.
Strength. The study’s design affords several notable strengths that enhance confidence in its findings. Leveraging the TriNetX platform allowed us to assemble one of the largest real -world cohorts of older breast cancer survivors with and without dementia to date. Because TriNetX aggregates records from over 100 participating health systems, the resulting sample encompasses diverse patient populations and practice settings, which improves the generalizability of the results. Moreover, the use of rigorous statistical methods including one -to- one propensity score matching and adjustments for a comprehensive array of demographic, clinical and medication variables which helped minimize confounding and ensured that the observed associations were not driven by imbalances between cohorts. Our precise outcome definitions, which incorporated multiple International Classification of Diseases codes (ICD-code) for fall events, captured a wide spectrum of falls from single incidents to recurrent episodes and fall- related injuries. This approach aligns with broader evidence that cognitive impairment markedly increases fall risk: older adults with dementia fall two to three times more frequently than cognitively healthy peers, and between sixty and eighty percent of individuals with dementia fall each year. These methodological strengths yield robust, broadly applicable insights into fall risk among this medically complex population. The Kaplan Meier survival analysis provided an unadjusted age-based estimate of fall-free survival, illustrating the cumulative incidence of falls over time before accounting for other covariates in multivariable models.
Limitation. Several limitations should be considered when interpreting the results. The retrospective nature of electronic health record analysis precludes causal inference and relies on accurate coding. Falls that did not result in medical attention were not captured, potentially underestimating the true incidence of fall events. Although we adjusted for many potential confounders, residual confounding may persist because data on certain factors such as the severity and type of dementia, detailed cancer treatments, functional status or living environment were unavailable. Additionally, although the outcome definition captured both single and recurrent falls, recurrent falls were not analyzed as a separate longitudinal outcome, which may warrant further investigation because repeated falls may reflect distinct intrinsic risk mechanisms. The “unspecified dementia” category used here includes heterogeneous etiologies, which prevented us from examining how different dementia subtypes might influence fall risk. Additionally, while TriNetX provides a large and diverse sample, its composition may not fully represent populations outside North America, and coding practices may vary across contributing institutions, introducing some misclassification bias. These factors highlight the need for future prospective studies with more granular data to confirm and extend the current findings.
Among older breast cancer survivors, dementia was associated with substantially elevated fall risk independent of age, frailty, neurologic comorbidity, depressive symptoms, and medication burden. These findings suggest cognitive status may be an important yet underrecognized component of fall risk stratification in survivorship care. Incorporating dementia related vulnerability into screening and prevention efforts may help identify survivors at heightened risk and support more targeted multidisciplinary interventions. Future longitudinal studies should further clarify mechanisms linking cognitive decline and falls and inform prevention strategies in this growing population.
This retrospective study used deidentified electronic health record data extracted from the TriNetX network at Virginia Commonwealth University Health System. The study was reviewed by the Virginia Commonwealth University Institutional Review Board and was classified as not human subjects research because the analysis involved deidentified data and did not include direct participant contact or access to identifiable private information. Therefore, ethical review and approval were waived, and formal IRB approval was not required.
Informed Consent Statement. Patient consent was waived because the study used deidentified electronic health record data and did not involve direct participant contact, intervention, recruitment, or access to identifiable private information.
Trial Registration. Not applicable. This study was not a clinical trial.
Declaration of Helsinki STROBE Reporting GuidelineThis study was conducted in accordance with the principles of the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline was followed.
The data that support the findings of this study are available upon reasonable request. Interested researchers can obtain access to the data by submitting a formal request to the corresponding author. The data is not publicly available due to privacy or ethical restrictions.
AN conceptualized the study, designed the analysis framework, conducted the TriNetX data extraction and statistical analyses, interpreted the findings, and drafted the manuscript. OP contributed to study conceptualization, data interpretation, and critical manuscript revision for intellectual content. FZ provided guidance on gerontology and aging-related interpretation, contributed to methodological refinement, and reviewed the final manuscript for accuracy and coherence. NT contributed to study design, methodological development, interpretation of findings, critical revision of the manuscript for intellectual content, and overall research supervision.
The authors declare that there are no conflicts of interest regarding the publication of this paper. None of the authors have any competing financial or non-financial interests in relation to the work described. This includes no direct relationships such as employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding that could influence the work reported in this manuscript.
This work was supported by the Wright Center under the Clinical and Translational Science Award (CTSA) Grant number UM1TR004360.
We extend our gratitude to the informatics team at Virginia Commonwealth University’s (VCU) C. Kenneth and Dianne Wright Center for Clinical and Translational Research, especially Tamas Gal and his team members, Evan French and Patrick Shi, for their invaluable support in data extraction through TriNetX platform.
1.
2.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions





