Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(3):e260017. https://doi.org/10.20900/agmr20260017
 ,
Beth Fields 2 ,
Danielle L. Wild 2 ,
Rylie A. Hechel 2 ,
Madeline G. Miller 2
,
Beth Fields 2 ,
Danielle L. Wild 2 ,
Rylie A. Hechel 2 ,
Madeline G. Miller 2
1
2
*
Background: Most older adults want to age in place, but many homes are not safe or accessible. Evidence-based aging in place interventions such as the Community Aging in Place Advancing Better Living for Elders (CAPABLE) program include home modifications as a key component but the specific impact of such modifications on home accessibility for older adults is poorly understood. Method: A secondary analysis of home accessibility was completed with data collected using Home for Life Design® for a single group pre/post cohort CAPABLE parent study conducted in Pennsylvania, U.S.A. CAPABLE is an evidence-based interprofessional intervention delivered by an occupational therapist, a registered nurse, and handy worker. The intervention includes up to 10 visits to the participants’ homes to assess accessibility, recommend modifications, and provide strategies to enhance independence and safety. Participants were recruited through an Area Agency on Aging and included in this study if they met the parent study’s inclusion criteria and completed both pre- and post-intervention home accessibility assessments. During the first and final occupational therapy intervention visits, the occupational therapist administered the Home for Life Design® assessment to gather an Accessibility Ratings™ (AR) score. Results: Forty-four participants were included in this secondary analysis. The CAPABLE intervention was associated with significant, large improvements in home accessibility ratings (Z = −5.45, p < 0.001). Median accessibility scores increased by 19.80% from pre- to post-intervention following home modifications (pre = 58.55% and post = 78.35%). Conclusion: The CAPABLE intervention may improve home accessibility, which may help older adults maintain independence and age in place. Results should be interpreted with caution due to lack of a comparison group, convenience sampling and potential assessor bias.
The world is growing old. Advances in healthcare continue to promote longevity, and the population of older adults (aged 65 or older) grows steadily each year, currently exceeding 61 million individuals in the United States and 830 million older adults worldwide [1,2]. Many older adults have a strong preference to remain in their homes forever [3,4]. Indeed, eighty percent of older adults indicate their goal is to age in place [3]. Aging in place is characterized by living in one’s home and community throughout the lifespan [5]. Previous research has found that remaining in the home provides older adults with a sense of familiarity, comfort, purpose, and connection to the greater community [4]. Higher life satisfaction and increased quality of life are also associated with aging in place [6–8]. Despite these benefits, environmental barriers can significantly limit older adults’ ability to stay in their homes [3].
Environmental barriers within the home can limit accessibility, which is defined as features in the home environment that promote both independence and safety, and can lead to an increased risk of falling [9,10]. This is often described in aging in place literature as a poor person-environment “fit” [11,12]. For older adults, falls are the leading cause of injury-related death [13] and are often the catalyst for moving into assisted living facilities [14]. The majority of falls occur in living spaces such as bedrooms, stairs, or bathrooms [15]. Accessible home design features, including no-step entries, handrails, grab bars, and accessible floorplans can support independent and safe living [16]. However, most homes do not meet the accessibility needs of individuals with movement-related disabilities or mobility devices [17]. Due to the scarcity of accessible home design and the desire of older adults to age in place, it is imperative to both identify and reduce fall-contributing accessibility factors in the home. Evidence strongly supports the use of fall-prevention education [13] and home modifications to improve accessibility [18]. While this process can vary from setting to setting, modifications such as improving lighting, adding grab bars, securing or removing throw rugs, decreasing clutter, and adding bright paint for increasing contrast are suggested ways to increase home safety and accessibility [15]. Aging in place interventions may offer a solution, supporting the implementation of home modifications that promote older adults’ engagement in meaningful everyday activities while simultaneously reducing fall risk.
One intervention that utilizes home modifications to improve the accessibility of older adults’ homes is the Community Aging in Place Advancing Better Living for Elders (CAPABLE). CAPABLE is a well-established evidence-based intervention demonstrated through a large randomized controlled trial to reduce disability in activities of daily living (ADL), reduce falls risk, and promote aging in place. [19,20]. As a preventative care model, the implementation of CAPABLE has reduced healthcare costs, reduced hospital admissions, delayed nursing home admissions and become an exemplar for global budget models of healthcare and population health [21,22]. CAPABLE is an interprofessional, person-centered intervention that involves occupational therapists, registered nurses, and handy workers to improve person-environment fit [11,12]. To deliver CAPABLE, occupational therapy and nursing interventionists must first complete a robust, online training which includes a manualized approach and clear intervention fidelity guidelines [19]. The intervention is delivered over four months with up to 10 home visits, six visits with the occupational therapist and four visits with the registered nurse. The occupational therapist assists the older adults in setting functional goals and modifying their behaviors to promote independence and safety within their home environment [20,23]. As a key component of this work, the occupational therapist conducts a home evaluation to identify environmental barriers that limit accessibility, recommending up to $1300 in home repairs and modifications for the handy worker to complete. In addition to reducing healthcare spending, CAPABLE promotes autonomy and independence for older adults and increases community engagement to improve their quality of life and safety in their homes [20,23].
Past research has demonstrated that CAPABLE removes barriers in ADL and instrumental ADL(IADL), increases confidence to complete ADLs and IADLs without falling, and decreases depression and pain symptoms [24].However, only one study has closely examined CAPABLE's impact on environmental barriers within the home[25]. While results supported a decrease in home hazards and improvement in overall safety following the intervention, interpretation of these findings were limited due to data collection using a non-standardized, general home safety checklist with limited capacity to assess changes in hazards before and after CAPABLE [25]. Such checklists are easy to use but may overlook potential environmental barriers revealed through performance-based assessment, [26,27] and lack a standardized method to collect and analyze data to produce, measurable outcomes[28]. While CAPABLE does require assessment of the home to identify needed home modifications, the intervention does not mandate the use of a standardized measure to evaluate home accessibility [19].
Therefore, the aim of this study was to determine the impact of the CAPABLE intervention on older adults’ home accessibility using a standardized, performance-based assessment tool called the Home for Life Design® (HFLD). We hypothesized that participants would demonstrate improved home accessibility following the CAPABLE intervention, as evidenced by higher post-intervention Accessibility Rating™ scores compared to baseline.
This secondary analysis utilized data from the parent CAPABLE study–a pragmatic hybrid type 1 trial testing the implementation of an established, evidence-based aging in place intervention within a home and community-based service agency [29] and employed a one-group pretest-posttest design to examine changes in participants’ Accessibility Rating™ scores before and after the CAPABLE intervention.
Ethical ConsiderationThe University of Pittsburgh Institutional Review Board (IRB) approval was obtained for the parent CAPABLE study (Study number 19090268 approved January 24, 2020). Informed consent was obtained from all subjects involved in the parent study. This secondary analysis used de-identified data and therefore did not require separate IRB approval.
ParticipantsThe CAPABLE intervention recruited older adults through the Allegheny County Area Agency on Aging (AAA) located in Western Pennsylvania, U.S.A. Specifically, the study targeted older adults who were eligible for or receiving home and community-based services but were above the financial threshold to qualify for these services without cost through Medicaid. To be eligible, the older adult participants had to: (1) be 60 years of age or older, (2) live in a house or apartment (3) have at least two chronic conditions, (4) experience difficulty with one or more daily ADL/IADL, (5) be able to stand unassisted (or with the use of a cane or walker), (6) and have a care partner (family member or friend) that supports them. Additionally, for this secondary analysis, participants were included only if they had complete pre- and post-intervention scores on the HFLD assessment. Participants were excluded from the study if they were (1) nursing facility clinically eligible but living in the community (2) actively receiving Medicare (skilled) home health, (3) actively receiving treatment for cancer, or (4) had a dementia or Alzheimer's diagnosis.
Older adults interested in learning more about the study were contacted via phone by a research team member. A brief screening was administered to collect AAA referral information and confirm eligibility, utilizing four questions from the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR) [30]. Participants were required to answer at least 2 questions correctly to ensure cognitive competence before proceeding with study enrollment.
MeasuresHome for Life Design® (HFLD). HFLD is a metric driven, web-based tool used to evaluate home accessibility during ADL/IADL performance [31]. HFLD users must register with HFLD site to gain access to the tool. Training materials include training videos, case stories, scoring decision guides and a series of frequently asked questions. Outcome scores and descriptive information are electronically generated upon pre and post data input via the HFLD website [31]. Rooms selected for assessment are person-centered and determined by the functional goals identified with the older adult. Based on the older adult’s occupational performance, HFLD administrators rate accessibility for each selected room on a scale from 0 (client cannot perform function; not accessible) to 10 (client can perform function safely; fully accessible), with 5 indicating partial accessibility client can perform function, but there are still barrier(s) to address [32]. For example, in the bathroom, ratings consider tasks such as transferring to the toilet and/or bathtub, retrieving items from cabinets, and maneuvering in the bathroom. The HFLD generates an Accessibility Rating™ (AR) for each room assessed (e.g. kitchen, bathroom, living areas, entryways, and bedroom), reported as a percentage, with higher scores indicating greater accessibility. Previous studies demonstrated excellent interrater reliability (intraclass correlation coefficient = 0.93) and strong content validity (content validity index = 0.875–1.00) for the HFLD assessment [33,34].
ProceduresBefore starting the CAPABLE intervention, a research team member met with the participants in-person to obtain written informed consent and gather demographic information (gender, ethnicity, age, education, relationship status, and income). During the first home intervention visit and following the CAPABLE guidelines, the occupational therapist completed the HFLD and determined if there were any environmental barriers that were preventing participants from independently and safely completing ADL/IADL. The occupational therapist used the HFLD for each room with the older adult to identify specific areas of concern and submitted a work order for necessary home repairs or modifications to be completed by the handy worker. During the subsequent visits, the occupational therapist and older adult (and their care partner if desired) collaborated to create modifications and compensatory strategies to complete selected ADL/IADL (i.e. bathing, grooming, cooking). Additionally, the occupational therapist educated the older adults on fall prevention and determined whether a referral to physical therapy for balance support was necessary. The RN completed up to four visits to educate the older adult on medical management, wound care, pressure sore prevention, and other medical needs. On their final intervention visit, the same occupational therapist conducted the HFLD again with the older adult to collect post-intervention data. Occupational therapy visits lasted approximately 1 to 2 h.
Data AnalysisAll data were deidentified by assigning a subject ID number to each participant. Data were stored securely in Research Electronic Data Capture (REDCap) [35]. Descriptive statistics were used to describe the sample. During data analysis, AR scores across all assessed rooms were averaged for each participant and analyzed using the Statistical Package for the Social Sciences (SPSS) Statistics Version 29.0 [36] to assess changes in home accessibility. A box plot identified one outlier in the post-intervention dataset, which was retained after determining it was a valid data point. Normality was tested using the Shapiro-Wilk test, which indicated the data were not normally distributed (p > 0.05). Because assumptions for a paired t-test were not met, a non-parametric Wilcoxon Signed-Rank Test was conducted to establish pre- and post-intervention changes in accessibility.
Power CalculationFor the parent study, a power analysis was conducted with a desired alpha level of 0.05, a power of 0.95, and an effect size of 0.5 to determine the required sample size. The power analysis suggested that 45 participants were needed to detect significant changes resulting from the intervention.
Of the 90 older adults enrolled in the parent study, 44 participants had complete pre- and post-home HFLD assessment data and were included in this secondary data analysis. Participants were excluded due to hospitalization, loss to follow-up, receipt of home health services, relocation, or death. There were no significant differences in baseline characteristics between included and excluded participants. Participants were predominantly female and white, with a mean age of 78.0 years, and a majority of participants reported an annual income of less than $25,000. See Table 1 for additional demographic information. The most common rooms assessed by occupational therapists were bathrooms, kitchens, living rooms, and primary bedrooms.
Table 2 presents the number of rooms analyzed, the percentage of participants with each room type assessed, and mean AR scores at baseline and follow-up. Across all room types, mean AR scores improved following the intervention.
As shown in Figure 1, 90.9% of participants demonstrated improvement in AR scores following home modifications. Median AR scores increased from 59.0% at baseline to 78.5% at follow-up, representing a median change of +20% (IQR = 15.5%). This improvement was statistically significant (Wilcoxon signed-rank test: Z = −5.45, p < 0.001) and associated with a large effect size (r = 0.581). The 95% confidence interval for the median change, estimated using bootstrap resampling, ranged from 14.0% to 23.0%, indicating a clinically meaningful improvement in home accessibility following the intervention.
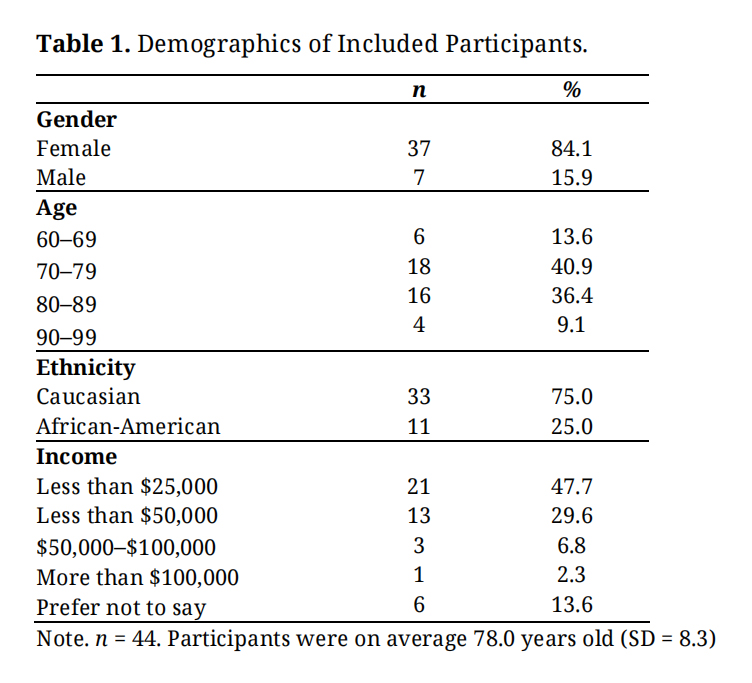 Table 1. Demographics of Included Participants.
Table 1. Demographics of Included Participants.
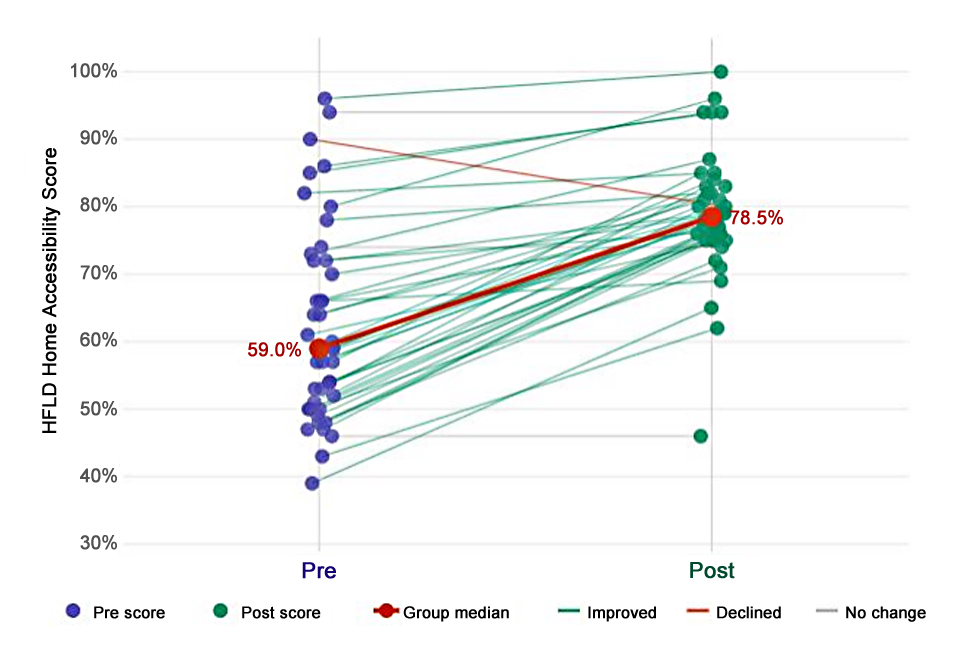 Figure 1.
Pre- and post-intervention scores for individual participants (n = 44). Each circle represents one participant’s score at pre-intervention (purple) and post-intervention (green), connected by a line coloured by direction of change: green = improvement, red = decline, grey = minimal change (≤2 points). The orange line and filled circles indicate the group median at each time point. Pre-intervention median = 58.5%, post-intervention median = 78.0%.
Figure 1.
Pre- and post-intervention scores for individual participants (n = 44). Each circle represents one participant’s score at pre-intervention (purple) and post-intervention (green), connected by a line coloured by direction of change: green = improvement, red = decline, grey = minimal change (≤2 points). The orange line and filled circles indicate the group median at each time point. Pre-intervention median = 58.5%, post-intervention median = 78.0%.
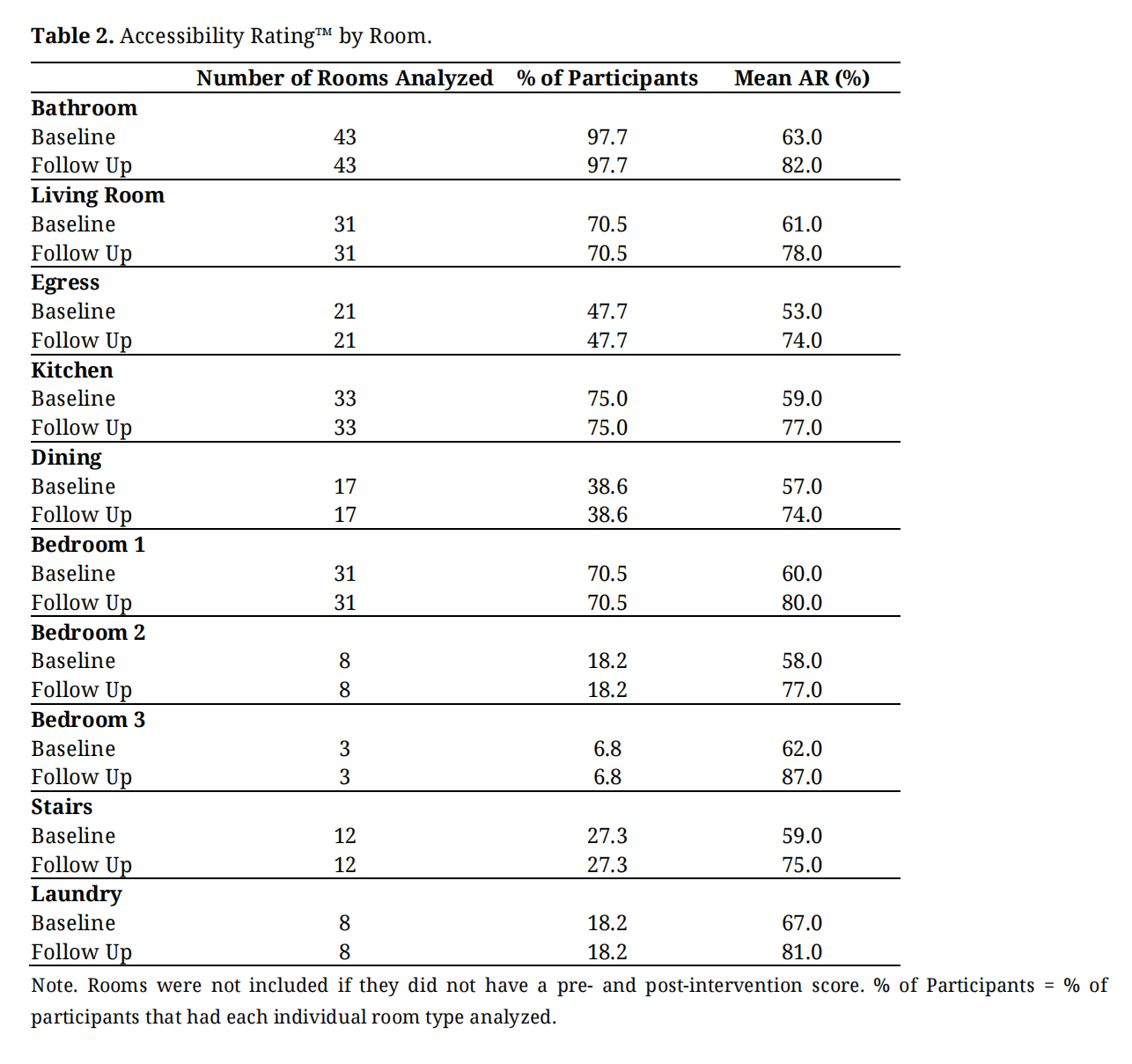 Table 2. Accessibility Rating™ by Room.
Table 2. Accessibility Rating™ by Room.
The findings of this study support our hypothesis that participation in the CAPABLE intervention would lead to significant improvements in home accessibility as measured by the HFLD. Positive changes in accessibility scores were found across all room types (kitchen, bathroom, bedroom, etc.). Results suggest that the CAPABLE intervention may be a feasible solution for increasing accessibility within the home environment, which could positively impact older adults’ ability to remain independent and safe in their homes.
Our findings align with prior evidence suggesting the efficacy of CAPABLE through modifying the home environment [23–25]. However, to our knowledge, our research is the first study to evaluate changes in home accessibility during CAPABLE using a standardized, performance-based measure. Our findings extend and strengthen prior work that examined home environment changes following CAPABLE. For example, Breysse et al. (2021) [25] demonstrated that CAPABLE produced significantly greater reductions in home hazards than a comparison group that received fall-recovery education; however, their study relied on a non-standardized, home safety checklist. In contrast, the present study uses a standardized, performance-based metric of accessibility, allowing for more precise assessment of environmental changes specifically associated with client goals for the intervention.
Occupational therapists and other health and social service professionals who assess home safety often rely on quick, checklist-based tools rather than performance-based assessments to evaluate home accessibility [37–39]. Commonly used checklists such as the Centers for Disease Control and Prevention’s (CDC) “Check for Safety” home safety checklist [40] and Rebuilding Together’s Safe at Home Checklist [41] offer rapid screening of environmental hazards but are limited in ability to measure change. These checklists provide a binary series of yes/no items that identify potential dangers in the home environment [42], yet they rarely capture how older adults actually perform essential ADLs/IADLs within their environments [43]. As a result, important functional limitations may go undetected, particularly when environmental barriers subtly—but meaningfully—interfere with task performance [27,37,39,43].
In contrast, standardized performance-based assessment tools, such as HFLD, offer richer insight into the dynamic interaction between the older adults’ capabilities, their home environment, and the ADL/IADL most important to them in daily life. In a recent study examining changes in through the Department of Housing and Urban Development Older Adult Home Modification Program, national home modification program in the United States, HFLD was able to demonstrate a 52% average improvement in accessibility, affirming the value and impact of the home modifications provided [44]. HFLD generates standardized, quantifiable scores that can allow clinicians and researchers to more accurately monitor how modifications in home accessibility influence ADL and IADL performance. The person-centered HFLD which uses performance-based data to guide the HFLD assessment process is an added strength that may generate increased understanding of minimal clinically important differences that promote aging in place [45]. Incorporating such performance-based tools into CAPABLE and other aging in place interventions in the United States as well as other countries such as the United Kingdom, Netherlands, Denmark and Australia where restorative or reablement services similar to CAPABLE are offered may strengthen the identification of environmental barriers that impede daily functioning and provide a more precise basis for tailoring home modifications to support safe and independent living [46].
Several key strengths emerged from this study. First, the use of HFLD as a, performance-based assessment ensured consistent data collection through standardized procedures [28,34]. Because the HFLD includes direct observation of older adults completing ADLs and IADLs, the occupational therapists could more accurately identify specific environmental barriers that interfered with task performance. Second, the study benefited from a pre-post design, which allowed for a clear evaluation of changes in home accessibility following the intervention. Third, the study examined the real-world implementation of HFLD within CAPABLE, increasing ecological validity and supporting the generalizability of results to community-dwelling older adults. Finally, the high proportion of participants who demonstrated improved AR scores strengthens confidence that the observed effects were robust.
While there are notable strengths, this study is not without limitations. The parent study employed a hybrid type 1 study design with a single group pre/post cohort to explore effectiveness and implementation of CAPABLE in a novel “real world” context [47]. Lack of a comparison group and the fact that participants in the parent study were recruited through convenience sampling limit strength of the findings and restricts generalizability. In our study, the same CAPABLE occupational therapist who completed the HFLD pre and post assessments also delivered the intervention. Thus, and despite a standardized HFLD approach, potential for bias in post-intervention scoring may have contributed to the results. In addition, although the HFLD assessment has demonstrated content validity and reliability, further psychometric testing is needed to fully establish its measurement properties across diverse populations and settings. Finally, because the analysis focused on immediate post-intervention outcomes, it remains unclear whether improvements in home accessibility persist over time or continue to support safety and function as participants age in place.
CAPABLE addresses many of the barriers that prevent older adults from aging in place, such as home accessibility and limited functional participation in daily tasks, through its interdisciplinary, client-centered approach. This study found that average home accessibility as measured by HFLD significantly improved following completion of the CAPABLE intervention. Through implementing aging in place interventions such as CAPABLE, occupational therapists can assist older adults in maintaining purpose, increasing quality of life, and aging safely in their homes [4,6–8].
The University of Pittsburgh Institutional Review Board (IRB) approval was obtained for the parent CAPABLE study (Study number 19090268 approved January 24, 2020). Informed consent was obtained from all subjects involved in the parent study. This secondary analysis used de-identified data and therefore did not require separate IRB approval.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The dataset of this study is available from the authors upon reasonable request.
PET and BF designed and implemented the study. DLW, RAH and MGM under BF analyzed the data. PET, DLW, RAH and MGM wrote the paper with input from all authors.
The authors declare there is no conflict of interest.
This study was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90RTGE0002).
We would like to express our gratitude to the participants who completed CAPABLE. Additionally, we are grateful to our intervention team for delivering CAPABLE and to the research team members whose support was instrumental in recruitment and data collection.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
Toto PE, Fields B, Wild DL, Hechel RA, Miller MG. Impact of Community Aging in Place Advancing Better Living for Elders (CAPABLE) on older adult home accessibility using Home for Life Design®. Adv Geriatr Med Res. 2026;8(3):e260017. https://doi.org/10.20900/agmr20260017.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




