Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250014. https://doi.org/10.20900/agmr20250014
 ,
Gabriella Engstrom 1 ,
Mike Wells 1 ,
Scott M. Alter 1,2,3 ,
Lisa M. Clayton 1,2,3 ,
Timothy P. Buckley 1,2,3 ,
Joshua J. Solano 1,2,3 ,
Patrick G. Hughes 1,2,3 ,
Vibhor Agrawal 1 ,
Richard D. Shih 1,2,*
,
Gabriella Engstrom 1 ,
Mike Wells 1 ,
Scott M. Alter 1,2,3 ,
Lisa M. Clayton 1,2,3 ,
Timothy P. Buckley 1,2,3 ,
Joshua J. Solano 1,2,3 ,
Patrick G. Hughes 1,2,3 ,
Vibhor Agrawal 1 ,
Richard D. Shih 1,2,*
1 Charles E. Schmidt College of Medicine, Florida Atlantic University, FL 33431, USA
2 Department of Emergency Medicine, Delray Medical Center, FL 33484, USA
3 Department of Emergency Medicine, Bethesda Hospital East, FL 33435, USA
4 Spencer Fox Eccles School of Medicine, University of Utah, UT 84112, USA
* Correspondence: Richard D. Shih
Background: Falls are the leading cause of fatal and nonfatal injuries in the United States for adults aged 65 years and older. The objective of this study was to determine the impact of patient self-perceived concern about falling on subsequent primary care provider (PCP) follow-up in older emergency department (ED) adults who sustained a head injury from a fall.
Methods: This was a secondary analysis of a large prospective study which included patients aged ≥65 years who had sustained head trauma from a fall. Patients with penetrating injuries, injury >24 h prior to presentation, and transfer from another hospital were excluded. Participants were telephonically followed up 14 days after ED presentation. They were asked about their concern for a repeat fall and whether they had followed-up with their PCP since discharge.
Results: Of 1527 participants surveyed, 769 (50.4%) were concerned about falling again and 758 (49.6%) were slightly or not at all concerned. There was an overall low PCP follow-up rate. The follow up rate was slightly higher for those concerned vs. not concerned about falling (62% vs 56%, p = 0.035; OR = 1.25, 95% CI: 1.01–1.53).
Conclusions: Geriatric ED patients who suffered head injury from a fall and expressed concern about future falls were more likely to follow up with their PCP. Fifty percent of participants with a self-reported fall expressed little to no concern for falling again. This suggests that many ED patients that have fallen are vulnerable to deficient PCP follow-up and fall prevention strategies. We suggest increased physician and patient education to emphasize fall prevention and PCP follow-up.
Primary care provider (PCP); Emergency department (ED); research assistants (RA); Stopping Elderly Accidents, Deaths & Injuries (STEADI); The US Preventive Services Task Force (USPSTF); transitional care management (TCM)
Falls are the leading cause of injuries in the US for adults aged 65 years and older [1]. One in four older adults in the US fall annually, accounting for approximately 32,000 deaths, three million ED visits, and 950,000 hospitalizations [2]. Both fatal and nonfatal falls in the older adult population cost the US almost 51 billion dollars in healthcare expenditures annually [3]. Nonfatal falls, specifically, cost approximately 29 billion dollars for Medicare, 9 billion dollars for Medicaid, and 12 billion dollars for private or out-of-pocket payers. The growing number of Americans over 65 years will lead to a dramatic increase in falls, as well as their attendant hospitalizations and related costs.
Fall prevention in the geriatric population is challenging as there are many factors that contribute to fall-related injuries [4]. These include difficulty with implementation of exercise programs and/or physical therapy, lack of fall-risk assessment and utilization of fall-prevention strategies by physicians, and lack of implementation of home safety improvements. In addition, the patient’s own perception of recurrent fall risk may play a substantial role in the lack of success of fall-prevention strategies [5–7].
Patient engagement in their own treatment care plan is imperative to minimize future falls and injuries, and several frameworks serve as the foundation to this. The protection motivation theory proposes that individuals with a self-perceived health threat will undertake actions to avoid harm [8]. Additionally, the social cognitive theory proposes that human behaviors are influenced by an individual’s self-efficacy, or ability to engage in a certain behavior, and outcome expectations, or belief that doing so will result in the desired effect. Both theories operate together to propel patients to confidently and actively seek appropriate and necessary care, especially after falling.
However, previous work has shown that older individuals at risk for falling who perceive less risk of adverse outcomes from a fall are less likely to engage in behavior to prevent that fall [6].
Follow-up with a PCPs after a fall is vital to assess the physical, functional, and psychosocial aspects of the patient’s health [9]. In a study of 87 patients discharged home who presented to an ED with a fall-related injury, 71% spoke to their healthcare provider about falls [10]. Primary care provider follow-up allows for comprehensive fall assessment, discussion of fall prevention strategies, especially in elderly patients that have already sustained fall-related injuries, a very high-risk group for recurrent fall [7].
Fear of falling has been previously studied to assess recurrent fall risk. However, it has not been utilized to assess for rates of primary care provider follow-up [6,11–13]. A single question screening tool was chosen for this ED based study due to practical limitations that include time constrains, limited staff and the impracticality of more comprehensive screening instruments (i.e., the Falls Efficacy Scale (FES)) [11,13]. The rationale for this study is as follows: falls are the leading cause of injury among older adults in the United States, yet follow-up care and prevention strategies after an initial fall are often inadequate. Understanding whether a patient’s self-perceived concern about falling influences their likelihood of primary care follow-up could help identify opportunities to improve post-ED care. If concern about falling is associated with higher follow-up rates, it may serve as a simple screening tool to guide targeted interventions and enhance fall prevention efforts among high-risk older adults. Therefore, this study aimed to determine whether concern about falling—assessed using a single-question screening tool—was associated with primary care follow-up among older adults who presented to the emergency department with a fall-related head injury. Understanding this relationship could help inform fall prevention education and support more patient-centered strategies to reduce recurrent falls and related injuries.
With this knowledge, fall prevention education and patient-centered approaches can be advanced, with the hope of reducing recurrent fall and fall-related injuries.
This investigation was a secondary analysis of data collected in a one-year prospective cohort descriptive study at two level-one trauma centers, beginning in August 2019. Both facilities are the only trauma centers serving the same county in Florida, with ED annual volumes of 50,000 and 69,000 patients respectively. The research committee of the participating hospitals and the university institutional review board approved the project. The primary outcome measure was PCP follow-up rates within the 14-day period after ED discharge.
ParticipantsInclusion criteria were ED patients aged ≥ 65 years who suffered head trauma following a fall. To ensure identification of all head injury patients, all ED Head CTs and ICD codes for head injury (S00 to S09) were screened. Exclusion criteria were patients who did not complete the 14-day follow-up call, patients with penetrating injuries, or injury more than 24 h prior to presentation, mechanism of injury other than from a fall, or transfer from another hospital.
Data CollectionTrained RAs performed structured chart reviews from hospital records and follow-up telephone interview in English, Spanish, or Haitian Creole after ED presentation with enrolled study participants. The initial follow—up call was made on or about 14 days after discharge from the hospital (with registration day taken as day 1). Although there is no specific recognized guideline related to the time to follow up with a PCP after a fall, the CDC Stopping Elderly Accidents, Deaths & Injuries (STEADI) program suggests “follow up for at risk patients in a timely manner” [https://www.cdc.gov/steadi/pdf/Steadi-Coordinated-Care-Plan.pdf accessed on 15 Sept. 2023]. We defined a 14-day period as a reasonable timeframe for follow-up, assuming that patients who intended to follow up because of their ED visit would do so within this “timely manner” window. If no response was received by the RAs on the first attempt, two subsequent attempts were made on different days and times of day. If the follow-up call was scheduled on a weekend or holiday, the call was completed the next business day or as soon as possible.
Prior to the start of the phone calls, RAs were educated on the conduction of human research trials and telephone interviews, with project co-investigators regularly available to provide feedback to the interviewers. All telephone interviews were conducted from a hospital telephone number and a voicemail was left if unanswered. Demographic and clinical characteristics were collected by the RAs from the hospital records.
VariablesData collected included mechanism of injury, age, race, sex, and comorbidities. Fall concern: patients were screened for fear of falling using a single-item question (SIQ) which, in our hospitals, is routinely asked of all older adults presenting to the ED. The participants were asked: “How concerned are you about falling again?” and given four options of “not concerned”, “slightly concerned”, “moderately concerned”, or “extremely concerned”. SIQ systems, while not as comprehensive as multi-question methods, can be considered appropriate for screening [14].
Adherence to PCP follow-up: Participants were asked: “Have you followed up with your primary care physician since being discharged from the hospital?” and given the options of “yes” or “no”. Those that responded in the negative, did not recall, or still planned to visit their PCP were included in the no follow-up group. Patients still planning to visit their PCP were included in the no-follow up group as, firstly, they might not attend follow up and, secondly.
Statistical AnalysisParticipants who were extremely or moderately concerned about falling again were grouped in the Concerned group while participants that were slightly concerned or not concerned at all, were grouped in the Not or Slightly Concerned group. The rationale for this grouping was that SIQ fear of falling screening systems have the highest agreement with validated scoring systems such as the FES in patients with higher fear of falling [15]. Although the 4-point SIQ that we used differed slightly from the methods evaluated by Belloni et al. and Meimandi et al., we felt it was likely that this association would hold true [11]. Demographic and clinical characteristics were compared according to classifications of fall concern and PCP contact follow-up. For each demographic and clinical characteristic, Pearson’s chi-square test was used for nominal variables and t-test analyses were used for normally distributed continuous outcome variables to examine the differences by groups. To address the primary outcome, the PCP follow up rate was calculated in each group of concern for falling. In addition, a multivariable logistic regression was used to address the influence of potential confounders on the association between patient concern about falling again and PCP follow up. The model included PCP follow up as the dependent variable and demographic factors, comorbidities, presenting signs and symptoms, and discharge location as the independent variables. All p values < 0.05 were considered indicative of statistical significance. Statistical analyses were performed using the IBM Statistical Package for the Social Sciences, version 27 (SPSS, IBM Corp, Armonk, NY, USA).
A total of 4951 patients presented to the ED for a fall with head injury, and 2962 were excluded for not meeting study inclusion criteria (Figure 1). 1989 patients were discharged from the hospital and included in the study. Of those, 462 (23%) did not consent to participation in telephone follow-up or could not recall a fall. There were 1527 participants ≥65 years that met study inclusion criteria. Of these, 769 (50.4%) were in the Concerned group and 758 (49.6%) were in the Not or Slightly Concerned Group (Figure 1).
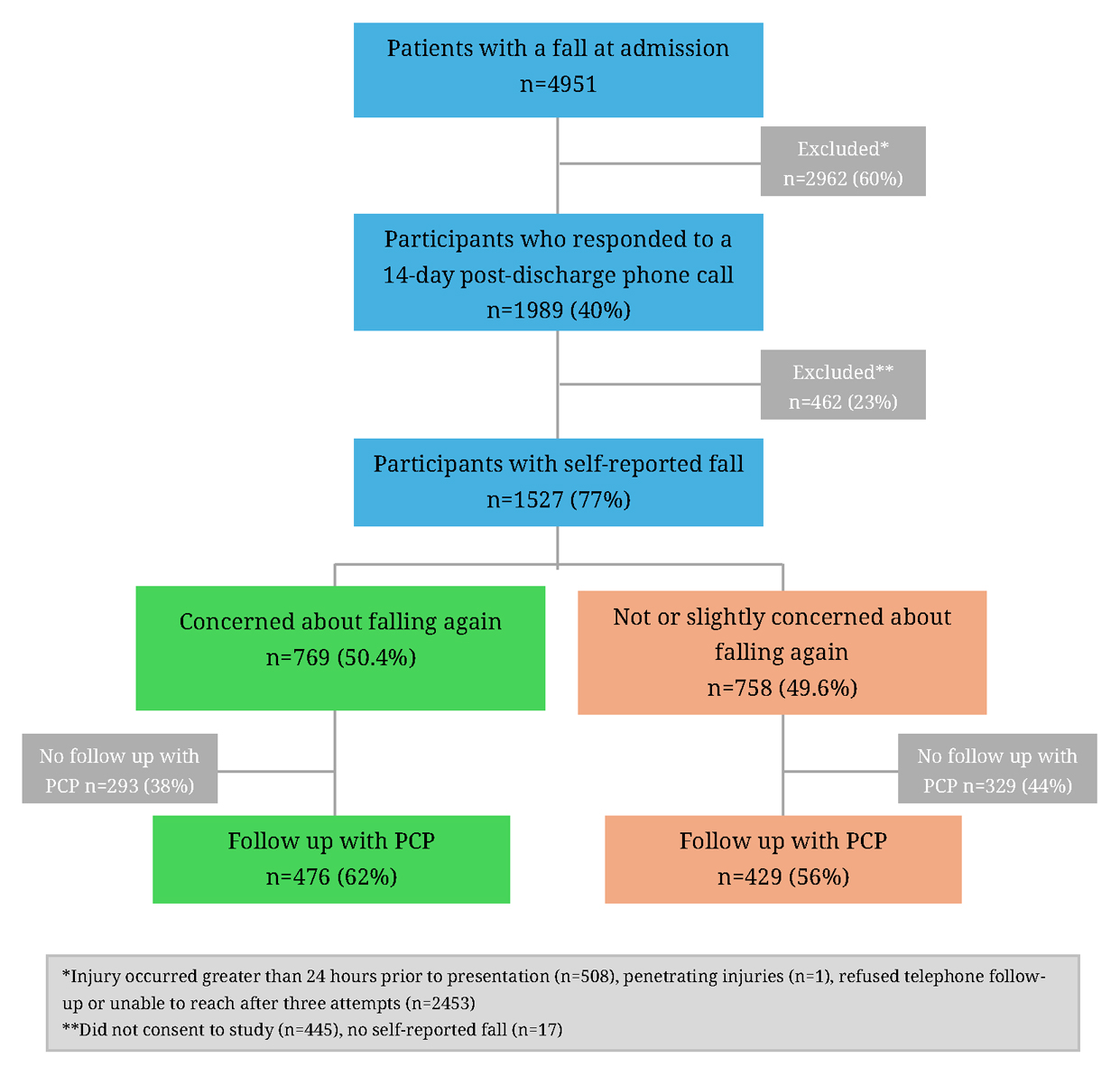 Figure 1. Flow Chart.
Figure 1. Flow Chart.
The demographic and clinical characteristics of the participants can be found in Table 1. Patients who were concerned about falling again were significantly older in age (83.0 vs. 81.2 years, p < 0.001). Additionally, a significantly greater percentage of participants with a fall concern, compared to those who were not or were slightly concerned, had hypertension (61% vs. 55%, p = 0.01; OR = 1.31, 95% CI: 1.07–1.60), diabetes (22% vs. 15%, p < 0.001; OR = 1.60, 95% CI: 1.23–2.08), atrial fibrillation (23% vs. 18%, p < 0.05; OR = 1.31, 95% CI: 1.02–1.69), dementia (11% vs. 7%, p < 0.01; OR = 1.71, 95% CI: 1.12–2.43), cerebrovascular attack (9% vs. 5%, p < 0.01; OR = 1.87, 95% CI: 1.24–2.81), chronic obstructive pulmonary disease (7% vs. 4%, p = 0.01; OR = 1.85, 95% CI: 1.16–2.97), and pulmonary embolism (2% vs. 0.5%, p < 0.01; OR = 4.26, 95% CI: 1.43–12.72).
Of the concerned fall participants, 476 (62%) followed up with their PCP after discharge from the hospital, while 429 (56%) of the not at all or slightly concerned fall participants followed up with their PCP. There was a significant association between PCP follow-up rate for those concerned vs. not at all or slightly concerned (62% vs 56%, p < 0.05). We also compared the group of patients with “No Concern” (226/416 (54%)) against those with any degree of concern about falling (679/1111 (61%)). There was a statistically significant difference between the groups OR 1.32 (1.05, 1.66) p = 0.019.
The results of the multivariable logistic regression analysis (controlling for age, gender, race, ethnicity, marital status, atrial fibrillation, cancer, cerebrovascular attack, chronic obstructive pulmonary disease (emphysema, chronic bronchitis), coagulation disorder, coronary artery disease/cardiac stent, congestive heart failure, deep venous thrombosis, dementia, diabetes, hypertension, peripheral vascular disease/peripheral stent, transient ischemic attack, pulmonary embolism, and valve replacement) revealed a virtually unchanged adjusted odds ratio for concern of falling again of 1.24 (1.01, 1.52) p = 0.043. This suggests that this is an independent predictor of PCP follow up. The only other statistically significant predictors among the comorbidities were cancer diagnosis (aOR 1.51 (1.1, 2.08)), hypertension (aOR 1.28 (1.04, 1.58)), and COPD (aOR 0.61 (0.39, 0.97)). In addition, presenting signs and symptoms and ED disposition location (admission, discharge) showed no significant association with patient follow up with PCP.
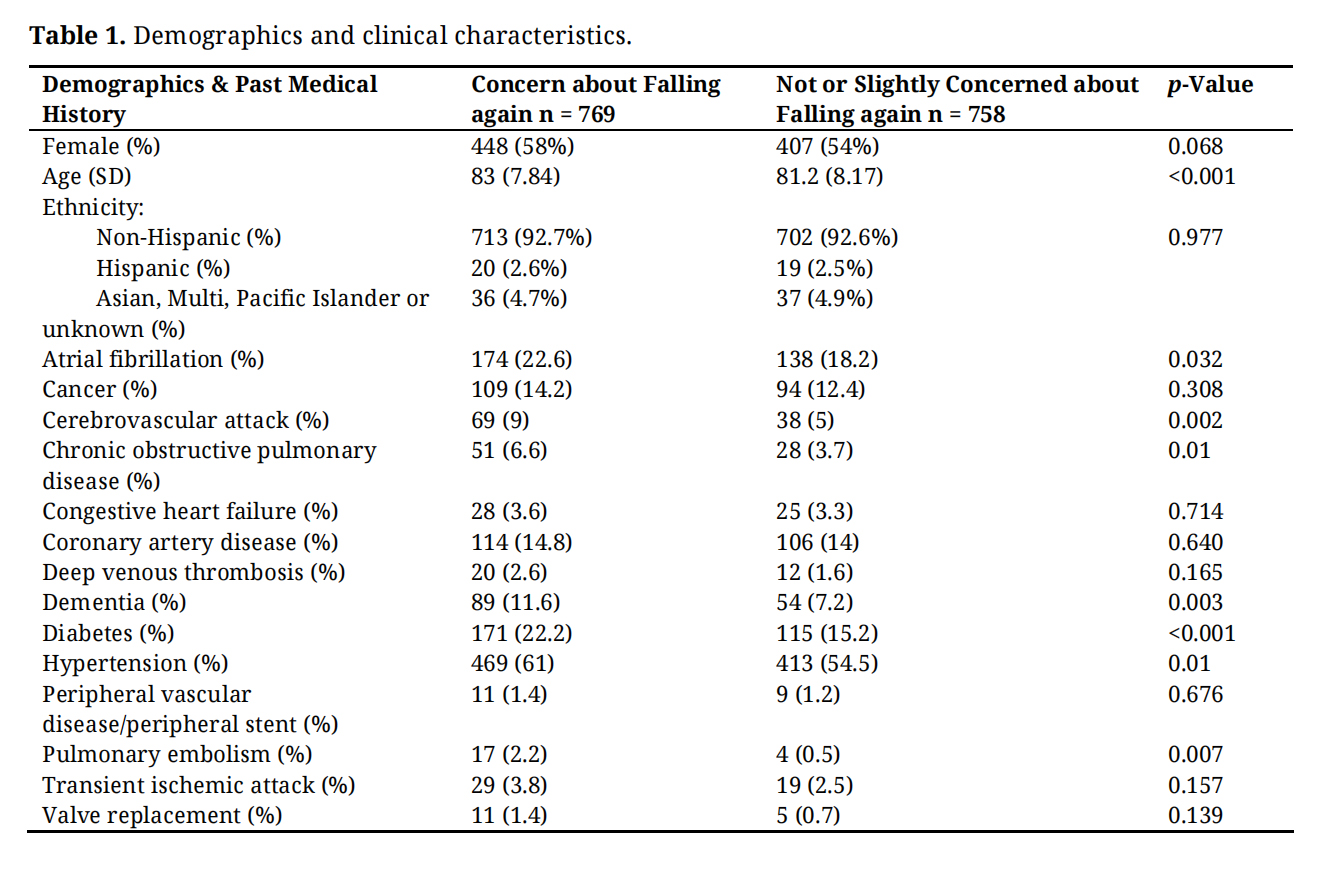 Table 1. Demographics and clinical characteristics.
Table 1. Demographics and clinical characteristics.
This study examined whether older adults’ concern about falling, measured by a SIQ, was associated with follow-up with PCP follow up after an ED visit for head trauma due to a fall. Three key findings emerged: about 40% of patients did not follow up with a PCP in a timely manner (within 14 days); fully half of the participants expressed little or no concern about falling again, despite having just experienced a significant fall-related injury; and patients with moderate to high concern about falling were approximately 25% more likely to seek PCP follow-up—suggesting that concern was a modest but significant predictor of engagement in follow-up care.
When viewed together these findings indicate a disconnect between actual and perceived fall risk. These patients are at high risk for recurrent falls but are less likely to receive appropriate follow-up and fall prevention interventions. Keeping patients engaged in their own healthcare is a key objective of quality and safety initiatives in the US [16]. The protection motivation theory, the basis for patient engagement, proposes that individuals with a self-perceived health threat will undertake actions to mitigate or prevent these threats [8]. However, in a study exploring patients with a high risk of fall related injuries, 88% of hospitalized patients reported not feeling at risk for falls [17]. Additionally, no association existed between perceived fall risk and actual fall risk, revealing that older adult patients likely lack the ability to accurately assess their fall risk. In a similar study, acutely ill inpatients who had fallen who are at a high risk for recurrent fall-related injuries, reported decreased intentions to engage in fall-prevention behaviors, which significantly correlated with their decreased fear of falling [6]. Patients carry their own set of beliefs and perceptions of fall risk, perhaps due to fear of vulnerability, denial of aging, desire to maintain autonomy and independence, and lack of understanding [18].
Fall concern and falls are intertwined and can lead to decline in health status if not promptly identified. In that regard, fear of falling is at times a delayed, rather than immediate, reaction a patient experiences after a fall. In a study examining the relationship between falls and fear of falling, those who fell and initially expressed no fear were more likely to subsequently report such fear within 20 months compared to individuals that had not fallen [12]. This suggests that the development of a fall concern may be delayed and may lead to delayed initiation of prevention strategies. For the nearly 800 slightly or not at all concerned older adults in our study, their physiological status and recent fall puts them at high risk for repeat fall, injury, and return to the ED. This lack of concern for additional falls is extremely concerning but may not be reflective of delayed development of fear for falling.
The ED is a decisive point in the fall prevention process, and proper patient education in the ED is critical. The fast-paced nature of the ED limits how much time a health practitioner spends with a patient. Most physicians are focused on the diagnosis of acute injuries and are not aware of the “hidden impact” of head injury in older patients [19]. Most EDs do not have the time and resources to assess fall-risk and to initiate fall prevention strategies, relying on outpatient follow-up to complete these important tasks. Coupled with the lack of fall risk assessment and fall prevention training [13], this is an area that can be improved.
While a SIQ fear of falling assessment (“How concerned are you about falling again?”) is feasible for use in the ED, more comprehensive methods like the 16-item FES are not [11]. Although SIQ tools have not been validated to the extent of methods like the FES, they are widely used and have been shown to correlate reasonably with the FES in patients with moderate or high concern for falling. Since fear of falling is a significant predictor of future fall risk the use of a SIQ has an important potential role as an easy-to-use screening instrument in the ED. Some easy to implement interventions could include the use of internet resources to provide inexpensive additional educational materials for patients [20]. Indeed, the U.S. Centers for Disease Control and Prevention’s “STEADI” program provides brochures, graphics, and easy-to read fall prevention materials for patients and their caregivers [21].
Though their PCP may furnish them with details about their health and fall prevention strategies to incorporate in their daily routines moving forward [22], a large group of our study participants (41% overall) did not follow up with their PCP. The USPSTF concluded that exercise interventions and multifactorial interventions based on initial assessment of modifiable fall risk factors offer a net benefit in preventing fall-related morbidity and mortality [23]. Primary care physician follow-up allows for comprehensive fall assessment and screening and discussion of reliable fall interventions such as those recommended by the USPSTF.
With these factors in mind, two main questions arise: first, how can we get more patients to follow up with their PCP? Follow-up behavior is complex, multifactorial and influenced by numerous variables beyond concern for falling, including current health status, access to care, caregiver support, and health literacy. It was clear that many patients with high levels of concern about falling did not seek prompt follow up, which supports this viewpoint. This needs additional research to identify factors that might influence follow up, and to identify strategies that could address this to potentially reduce the risk of future falls. Second, does the observed disconnect between patient perception of risk (concern of falling) and actual risk of falling reflect a limitation in the assessment by the SIQ system, or is it because of other factors. Both SIQ and multi-question assessment tools have limitations in this regard. Since it is impractical in the ED to routinely screen patients with long questionnaires, it is an important aspiration to determine whether a simple self-reported concern about falling might serve as a practical and clinically useful signal of intent to engage in timely post-ED care. This also needs additional research to provide a clear answer.
Our study has a few limitations. First, we were unable to contact many of the study participants by phone, limiting our knowledge of their PCP follow-up status. Individuals that are unable to be contacted may have limited capabilities and resources and may be less likely to follow-up with their PCP.
Second, it was unclear whether patients followed up with their PCP specifically because of their fall or due to other underlying health conditions. There is no specific data to address this confounder, but when we controlled for the presence comorbidities, fear of falling remained an independent predictor of PCP follow up. Interestingly, only some comorbidities were drivers of follow up, so some unknown elements remain which need to be clarified in future studies.
Third, while our study focused on fall concern as a predictor of follow-up behavior, other unmeasured factors such as transportation barriers, limited social support, and absence of family caregivers may also play a critical role in influencing PCP follow-up.
Fourth, a SIQ tool was used to assess fear of falling. While there is supporting evidence for this type of fall risk screening, it may not be as accurate as more comprehensive tools. This may have resulted in some misclassifications and confounded the results. Our use of pooled risk strata (moderate and higher fear of falling identified with a SIQ correlate well with the FES-I) was an evidence-supported method to limit this potential bias.
Approximately 40% of geriatric ED patients who sustained a head injury from a fall and expressed moderate or high concern about future falls did not follow up with their PCP within 14 days. Patients with little or no concern about falling again had a small but significantly lower PCP follow up rate. These are important findings in a group of individuals at high risk for recurrent fall and fall related injuries. Future research is needed to help patients and physicians understand the serious nature of falling and high risk of recurrent falls. In addition, factors that contribute to the development of a fall concern need to be established. Finally, educating physicians and the public regarding the seriousness of falls, availability of fall prevention and the important role a PCP plays is needed.
The study was approved by the Institutional Review Board of Florida Atlantic University (protocol code 1326154-1 and approved January 15, 2019) for studies involving humans.
Data were collected from medical records and patient consent was waived was waived. Obtaining informed consent at the time of initial data collection was deemed impractical due to the nature of the study design. Prior to the telephonic interview, verbal consent for participation was obtained using a standardized script by trained research assistants.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The dataset of the study is available from the authors upon reasonable request.
Conceptualization, RDS, SMA and JJS; Methodology, RDS, SMA and JJS; Formal Analysis, GE and MW; Investigation, RDS; Resources, RDS; Data Curation, SMA, GE, and MW; Writing—Original Draft Preparation, MK; Writing—Review & Editing, GE, MW, SMA, LMC, TPB, JJS, PGH, VA and RDS; Supervision, RDS; Project Administration, GE; Funding Acquisition, RDS.
The authors declare that they have no conflicts of interest.
This research was funded by Florida Medical Malpractice Joint Underwriting Association’s Alvin E. Smith Safety of Health Care Services Grant (RFA #2018-01) for the project entitled “The Geriatric Head Trauma Short Term Outcomes Project”.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Khazem M, Engstrom G, Wells M, Alter SM, Clayton LM, Buckley TP, et al. Lack of fall concern and primary care physician follow-up in geriatric emergency department patients with head trauma from a fall. Adv Geriatr Med Res. 2025;7(3):e250014. https://doi.org/10.20900/agmr20250014.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




