Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(3):e250015. https://doi.org/10.20900/agmr20250015
 ,
Taketoshi Hatta 2 ,
Mariko Horii 2 ,
Takahiko Kimura 1 ,
Kimiko Kato 3 ,
Junko Hatta 4 ,
Yukiharu Hasegawa 1 ,
Akihiko Iwahara 2
,
Taketoshi Hatta 2 ,
Mariko Horii 2 ,
Takahiko Kimura 1 ,
Kimiko Kato 3 ,
Junko Hatta 4 ,
Yukiharu Hasegawa 1 ,
Akihiko Iwahara 2
1 Department of Health Sciences, Kansai University of Welfare Sciences, Kashiwara 582-0026, Osaka, Japan
2 Department of Psychology, Kyoto Women’s University, Kyoto 605-8501, Japan
3 Department of Psychology, Aichi Sykutoku-University, Nagakute 480-1146, Aichi, Japan
4 Department of Psychology, Aichi-Gakuin University, Nisshin 470-0195, Aichi, Japan
* Correspondence: Takeshi Hatta
Objectives: Building on prior findings that individuals who perceive themselves as younger than their chronological age report better subjective health, the present study aimed to investigate the relative contributions of cognitive and physical factors to subjective age perception using multiple regression analysis.
Methods: In Study 1, a total of 639 community-dwelling adults completed questionnaires assessing subjective health and age perception. Subjective age perception was quantified using the PDS (Proportional Discrepancy Score). In Study 2, multiple regression analysis was conducted with data from 551 participants to examine the relative influence of cognitive and physical variables on PDS.
Results: Study 1 demonstrated that individuals who felt younger than their chronological age reported significantly higher subjective health compared to those who felt older. In Study 2, among the variables examined, the Stroop effect size (a cognitive measure) and back muscle strength (a physical measure) were significant predictors of PDS.
Conclusions and Clinical Implications: Study 1 verified the association between feeling younger and higher subjective health. Study 2 indicated that declines in higher-order cognitive functions are closely related to subjective age perception, supporting the developmental perspective that such functions, which mature later in life, tend to decline earlier with aging. From a positive psychological standpoint, community health professionals are encouraged to promote interventions that help preserve higher-order cognitive abilities as a means to foster a younger subjective age.
In addition to chronological age—the objective measure of time since birth—individuals also possess a subjective age, a psychological construct reflecting how old they feel. In developmental psychology, it is well-established that adolescents tend to perceive themselves as older than their actual age, reflecting a desire for autonomy and maturity [1,2]. In adulthood, subjective age perception becomes more complex and is shaped by a wide range of sociocultural influences [3–5].
The study of subjective age has progressed through two major research waves. The first wave focused on developmental and cultural variations in subjective age perception. The second wave shifted attention toward the role of subjective age in health and psychological well-being, particularly among middle-aged and older adults [6–8]. This theoretical evolution aligns with the rise of positive psychology, emphasizing the role of self-perception and positive self-concept in promoting health and longevity.
In this context, recent studies have highlighted that feeling younger than one’s chronological age is associated with beneficial health outcomes, such as increased participation in physical activity [9,10], reduced chronic pain [11], and even lower medical costs in aging societies. These findings underscore the importance of incorporating subjective age perception into health-promoting strategies and interventions for older adults.
Building on these insights, health psychology has increasingly explored the psychological and physiological factors that contribute to a younger subjective age. Longitudinal cohort studies—such as the National Health and Aging Trends Study (USA), the Interdisciplinary Longitudinal Study of Adult Development (Germany), the Population-based and Inspiring Potential Activity for Old-old Inhabitants (Japan), and the Berlin Aging Study II (Germany)—have provided valuable data for analyzing how subjective age relates to cognitive and physical functioning.
However, several methodological and theoretical limitations remain in previous research. First, many studies implicitly assumed that feeling younger is inherently linked to a subjective sense of good health, without empirically validating this association. Second, most studies employed multiple regression analyses using various health examination variables as predictors of subjective age. Yet, the rationale for variable selection was often unclear, and the analyses lacked consistency in the number and nature of included variables. Third, from a cognitive psychological standpoint, prior studies often neglected the multidimensional nature of cognitive function—encompassing attention, memory, executive function, reasoning, language, and spatial cognition—and focused on only a narrow range of these domains [12,13]. Similarly, studies examining physical function typically relied on limited indicators such as grip strength or gait speed, without contextualizing these metrics within developmental trajectories of physical aging [14]. We systematically selected the test items based on the LiFO (Late-in First-Out) Proposal of evolutionary development, which posits that skills acquired later decline early during the aging process, as described below [15,16]. Furthermore, it has been pointed out that subjective age perception is influenced by culture, but most studies have focused on Westerners, and to our knowledge, there are only two academic papers that have focused on Japanese people [3,17]
Given these gaps, the present research was designed in two stages. Study 1 aimed to verify the assumed relationship between subjective age perception and subjective health awareness of modern Japanese elderly adults. After establishing this association, Study 2 implemented a regression analysis to investigate how various health examination variables—selected with theoretical justification and methodological transparency—contribute to subjective age perception. This two-step approach addresses prior shortcomings and offers a more robust framework for understanding the psychological and physiological correlates of subjective age.
Study 1 PurposeThe purpose of this study was to investigate whether individuals who feel younger than their chronological age report a more positive subjective HRQoL (Health-related Quality of Life) compared to those who feel older.
Method ParticipantsA total of 1735 individuals aged 40 years and older participated in the Yakumo Study, a municipal health examination program (with 616 participants in 2008, 593 in 2009, and 526 in 2011). Participants who did not respond to the subjective age question or who participated multiple times were excluded; in the latter case, only data from the first year of participation were used. After these exclusions, the final sample consisted of 639 participants (361 women and 278 men).
Subjective AgeParticipants were asked by local government officials to complete a self-administered questionnaire titled About Your Health as part of the health examination. The questionnaire assessed various aspects, including depressive tendencies, cognitive and behavioral patterns, daily habits, forgetfulness, eating behaviors, and subjective age. Subjective age was measured by the question: “Aside from your actual age, how old do you feel?” Respondents provided their answers in numerical form.
Subjective age was operationalized using the PDS, following Stephan et al. [18]. Although other indices exist (e.g., raw score or discrepancy value), the use of the PDS is recommended by Debreczeni and Bailey [6] and Rubin and Berntsen [2]. The PDS was calculated as:
PDS = (Subjective Age − Chronological Age) / Chronological Age
A more negative PDS indicates that the respondent feels younger than their actual age, while a positive score indicates feeling older.
In addition, participants completed a questionnaire administered by the orthopedics team, assessing mobility, bodily pain, and perceived health status, in conjunction with the HRQoL survey.
HRQoL (Health-Related Quality of Life)Subjective health perception was assessed using subscales from the HRQoL measure. HRQoL was evaluated via the Japanese version (Version 2) of the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) [19]. This instrument comprehensively assesses health and functional status across a wide range of populations, independent of age, disease, or treatment condition.
The SF-36 includes multiple items assessing eight health dimensions:
1.
2.
3.
4.
5.
6.
7.
8.
For this study, the “General Health Perceptions” and “Vitality” subscale scores were used as indicators of subjective health perception. We selected and analyzed these two subscales that are most relevant to subjective well-being and align with our main hypothesis based on positive psychology.
Results and DiscussionParticipants were classified into three groups based on their subjective age responses: those who felt younger than their chronological age (“feeling younger”), those who felt older (“feeling older”), and those who felt the same (“feeling same”). Table 1 presents the PDS, Overall Sense of Health, and Vitality subscales of HRQoL for the three groups. As a reference, a PDS score of −0.13 corresponds approximately to perceiving oneself as 8 years younger at age 60 and 9 years younger at age 70. Conversely, a PDS score of 0.048 reflects perceiving oneself as about 3 years older at age 60 and 4 years older at age 70.
To determine whether the “feeling younger” group exhibited higher scores in Overall Sense of Health (higher scores indicate better perceived health) and Vitality (higher scores indicate greater perceived vitality), independent-samples t-tests were conducted. Results showed that the “feeling younger” group scored significantly higher than the “feeling older” group on both subscales (Overall Sense of Health: t (531) = 2.89, p < 0.01; Vitality: t (531) = 2.69, p < 0.05). For reference, the comparison results for the other six subscales are as follows; Limitation (physical health): t (531) = 2.81, p < 0.05; Bodily Pain: t (531) = 3.13, p < 0.001; Physical Function: t (531) = 1.04, p > 0.05; Social Function: t (531) = 1.15; Limitation (Emotion): t (531) = 0.90, p > 0.05; Mental Health: t (531) = 2.32, p < 0.05). Limitation (physical health): t (531) = 2.81, p < 0.05; Bodily Pain: t (531) = 3.13, p < 0.001; Physical Function: t (531) = 1.04; Social Function: t (531) = 1.15; Limitation (Emotion): t (531) = 0.90, p > 0.05; Mental Health: t (531) = 2.32, p < 0.05). These findings suggest that a younger subjective age is strongly associated with better self-perceived health and vitality among middle-aged and older adults. In other words, adults who feel younger can be considered subjectively healthier and more vital. Therefore, identifying the factors that influence subjective age perception is crucial for developing effective health promotion strategies for this population. In short, feeling younger may be nearly synonymous with feeling healthy.
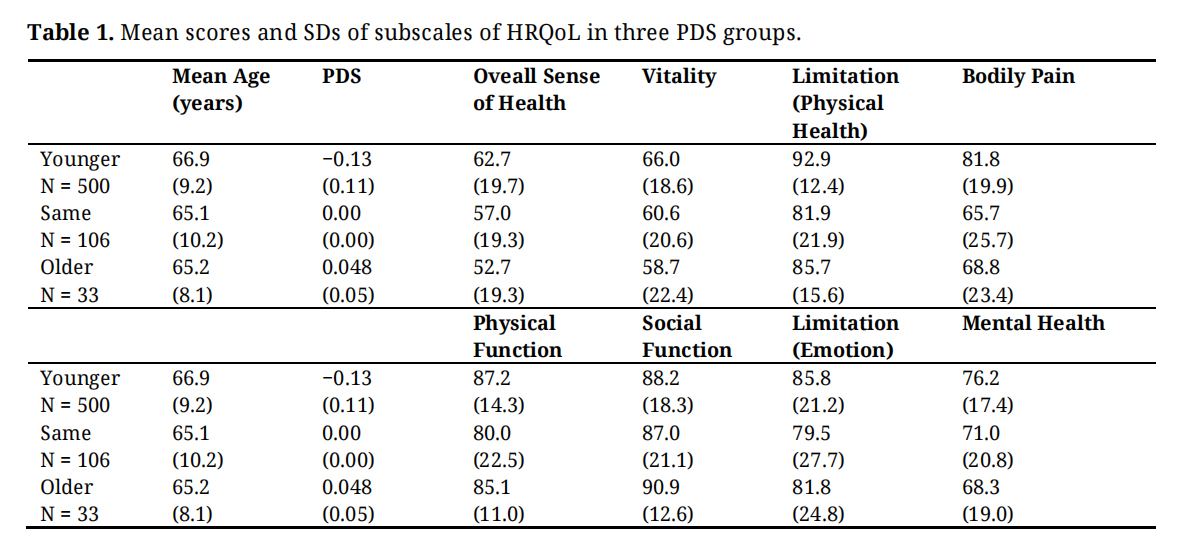 Table 1. Mean scores and SDs of subscales of HRQoL in three PDS groups.
Table 1. Mean scores and SDs of subscales of HRQoL in three PDS groups.
In this study, we aimed to identify cognitive and physical variables associated with subjective age perception, using assessment items from the Yakumo Study. Variable selection was guided by the theoretical framework of the LiFO Proposal [15,16], which posits that age-related cognitive decline reflects evolutionary development—functions acquired later in life tend to deteriorate more rapidly than those acquired earlier. Based on this perspective, it can be inferred that higher-order and more complex cognitive and physical functions are more vulnerable to age-related decline than simpler functions. Accordingly, we hypothesized that these higher-order functions would have a stronger influence on subjective age perception than lower-order functions.
Five hundred fifty-one community residents who participated in both the neuropsychological and orthopedic team examinations completed the questionnaire, of which 87% were participants in Study 1. For three years, many people participated in the neuropsychology (1259 participants) and orthopedics (1149 oarticipants) team examination, however, some did not respond to the questionnaire, some did not undergo examinations by both examination teams, and some received duplicate examinations. In the case of duplicate examinations, the results from the first year were used. To exclude participnts with suspected dementia, those with MMSE scores below 23 were excluded. Subjects with orthopedic diseases were excluded, and the used data were from a total 551 participants.
Demographic information is presented in Table 2. Although we noted mean years of education, it is unreasonable to assume a correlation between the length of education and cognitive function for participants born before 1948 in rural Japan. Therefore, unlike in Europe and the United States, this study did not include educational history in the analysis. The participants were considered community-dwellers with normal cognitive function drawn from a typical Japanese population with a history of employment in agriculture, fishing, forestry, and office work because Yakumo town has a typical structure in terms of the ratio of employment in the industrial structure that constitutes Japanese society.
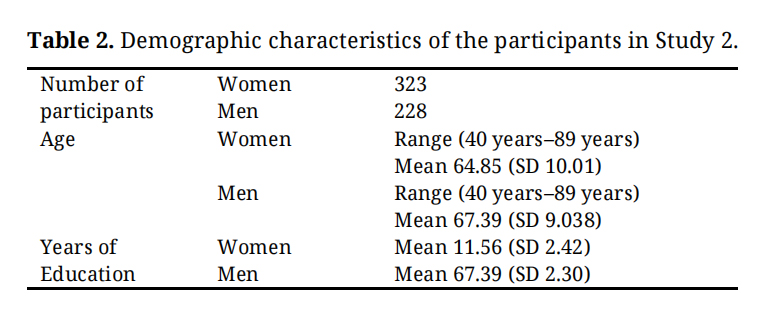 Table 2. Demographic characteristics of the participants in Study 2.
Table 2. Demographic characteristics of the participants in Study 2.
Independent variables consisted of the results from the neuropsychology and orthopedics teams in the 2008, 2009, and 2011 Yakumo Study. In the neuropsychology team examination, participants were given the NU-CAB (Nagoya University Cognitive Assessment Battery). The NU-CAB includes D-CAT (Digit Cancelation Test; assessment of information processing speed, focusing, and sustained attention), LMT (logical memory test; assessment of episodic memory), LFT (Letter Fluency Test; assessment of the verbal ability), SFT (Semantic Fuency Test; assessment of the verbal fluency), and Stroop test (assessment of executive function). We previously reported on the validity and reliability of the NU-CAB [20]. The NU-CAB originally included a Road Map Test (RMT, assessment of visuospatial ability), but it was not implemented in 2008.
The D-CAT test sheet comprised 12 rows of 50 digits. Each row contained 5 sets of numbers 0–9 arranged in random order. In the D-CAT, participants were instructed to search for the target number and delete each number with a slash mark as quickly and accurately as possible. In the LFT, participants were asked to generate as many nouns as possible beginning with syllables A, KA, and SHI, excluding proper nouns, numbers, and words previously instructed. In the SFT, participants were required to produce as many nouns as possible that belong to the assigned categories (animals, sports, and jobs) in 60 s. In the LMT, the examiner reads twice a short story from the WMS-R Japanese version [21] consisting of 25 segments, and each participant was asked to recall the story immediately. Each segment correctly recalled by the participant was given a score of 1 point; therefore, the total score ranged from 0 to 25 points. The Japanese version of the Stroop test was used [22]. A4-sized test plates were prepared for the control condition with 2.5 cm diameter circles in 8 rows and 5 columns printed in red, yellow, blue, and green, and for the Stroop condition, the words “red”, “yellow”, “blue”, and “green” were written in Chinese (Kanji) characters. The control condition consisted of reading the color name of dots in which four different colors were randomly arranged (dot condition). In the Stroop condition, there was a color mismatch between the color name and the ink color of the writing, which was thought to cause Stroop interference. The participant’s task was to read the color name as quickly and accurately as possible. The time required and number of errors were recorded. We used the measure where the time required in the Stroop condition divided by the time required in the dot condition was used as the Stroop effect size [23].
The data obtained from the orthopedics team included the MSL (Maximum Stride Length). On the starting line, put both feet together, take two steps with as wide a stride as possible, and measure the toes at the landing point twice in centimeters. The longer trial was used as the MSL of the participant. The 10MWT (10-Meter Walk Test) was used to assess walking speed. According to the guidelines recommended by the Clinical Practice Guidelines published by the US Academy of Neurologic Physical Therapy (ANPT), time measurements were carried out within 6 m, with the remaining acceleration and deceleration sections being 2 m each, for a total of 10 m. The participants walked 10-m both of “comfortable walking” and “fastest walking”, and the time taken was measured. The average of two measurements was used as the 10MWT score. The back strength was measured in 0.1 Kg units by using a back muscle strength meter and the balance ability, in addition to anatomical measures of body parts based on X-ray images, bone densitometer results, and pain examination. To assess balance ability, postural tremors were measured using a stabilometer (Anima GW 5000, Anima Co., Tokyo). Two examiners (an orthopedic surgeon and an assistant) measured the postural tremors of each participant. First, participants stood still for their 60 s with their eyes open, and then with an eye mask on, they were again asked to stand still for their 60 s. Participants placed their feet on the footprint of the device, stood upright with their arms down, and looked at a fixation point 2 meters away. The center-of-gravity sway while participants were standing upright was measured. Among the seven measurements for the open eye condition, the ENG/TIME (ENG) and ENV/AREA (ENV) scores were used because they are the most basic parameters of standing body balancing. The ENG is the length of the trajectory drawn per unit time by the center of gravity, and the ENV is the size of the area drawn by the trajectory.
As mentioned earlier, the number and quality of variables incorporated in a multivariate regression analysis are important because they significantly affect the results of the analysis. In this study, we decided to proceed with the analysis by adopting five cognition-related variables and five physical motor-related variables, considering the theoretical background. For this purpose, we incorporated the D-CAT, LMT, LFT, SFT, and Stroop effect size variables into the neuropsychology team examination. The MSL, 10MWT, ENG, ENV, and back strength scores were obtained from the orthopedics team data.
Dependent VariablesThe dependent variable was subjective age, as described in Study 1.
In Study 2, we investigated the factors associated with subjective age perception using both cognitive and physical variables. Although previous studies have applied various types of regression analysis due to recent advances in computation, many included health check-up items without adequate conceptual or numerical consideration in selecting variables. It should be noted that when calculating the relative contribution to subjective age using only cognitive or only physical variables as predictors, the results reflect associations within those respective domains. In contrast, the results differ when both cognitive and physical function variables are included as predictors, consistent with previous findings suggesting that subjective age is influenced by both cognitive and physical functions [24–27].
Therefore, in this study, we used multiple regression analysis to examine the relative contributions of cognitive and physical variables to subjective age perception. Based on the LiFO, five cognitive and five physical variables were selected, representing both lower-order (evolutionarily earlier) and higher-order (later-acquired) functions. The cognitive variables included D-CAT, LMT, LFT, SFT, and Stroop effect size. The physical variables, which reflect human physical development, included ENV, EGN, MSL, 10MWK, and back muscle strength. Among them, the Stroop effect size was assumed to represent higher-order cognitive function compared to D-CAT, while back muscle strength was considered a higher-order physical function relative to postural maintenance, ENV, EGN, MSL, and walking.
Ochsner et al. [28] employed an fMRI version of the Counting Stroop task and demonstrated that interference conditions strongly activated higher-order brain regions, particularly the anterior cingulate cortex (ACC), which are associated with executive functions and attentional control. This finding supports the interpretation that the Stroop task reflects a higher level of cognitive processing than simple visual-motor speed.
Similarly, Nagahara et al [29] conducted a cognitive aging study in older adults using both the Stroop task (reaction time) and the Digit Cancellation Test (D-CAT). Their results showed that only Stroop reaction time continued to decline with age, whereas D-CAT performance remained stable. This suggests that the Stroop task more sensitively reflects higher-order cognitive processes such as inhibition and cognitive control.
Regarding physical function, several studies have demonstrated that resistance training involving back muscle strengthening not only improves motor abilities but also enhances executive function and cognitive inhibition. For example, Liu-Ambrose et al. [30] reported that a 12-month resistance training program improved executive functions in older adults. Bolandzadeh et al. [31] further showed that increased muscle strength through resistance training was associated with better cognitive performance. Importantly, Best et al. [32] used fMRI to show that resistance training targeting the back muscles led to increased activation in the prefrontal cortex and ACC, indicating that improvements in back strength can influence neural circuits related to higher cognitive function.
Together, these studies provide converging evidence that (1) the Stroop task is a valid index of higher-order executive function, and (2) back muscle strength may reflect higher-level cognitive mechanisms, rather than merely lower-order motor functions such as postural maintenance, balance, or walking.
Table 3 presents the correlation coefficients among these variables. Most of the cognitive variables were significantly correlated with PDS, whereas among the physical variables, only MSL and back strength showed significant associations. Notably, gait- and posture-related variables were not significantly correlated with PDS. This pattern suggests that the association with subjective age may be driven by whether the physical activity involves non-automatic, consciously controlled movements—an essential component of executive function.
The results of the multiple regression analysis with PDS as the dependent variable are shown in Table 4. Among all variables, only Stroop effect size and back strength made significant contributions to PDS. Interestingly, cognitive variables that had significant bivariate correlations with PDS did not retain significance in the multivariate model. These results support the LiFO Proposal, indicating that higher-order functions are more vulnerable to age-related decline. Back strength, as a higher-order physical ability developed after walking and standing, similarly appears to influence subjective youthfulness.
Overall, these findings suggest that when middle-aged and older adults evaluate their own “subjective youthfulness,” they may do so based on introspective assessments of higher-level intellectual and physical capacities.
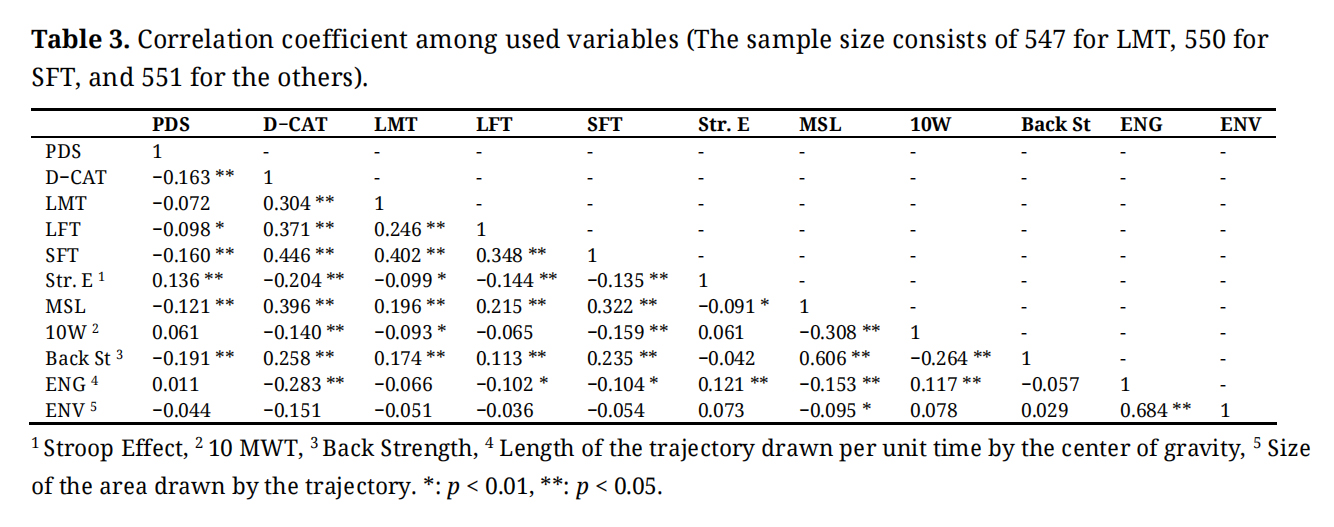 Table 3. Correlation coefficient among used variables (The sample size consists of 547 for LMT, 550 for SFT, and 551 for the others).
Table 3. Correlation coefficient among used variables (The sample size consists of 547 for LMT, 550 for SFT, and 551 for the others).
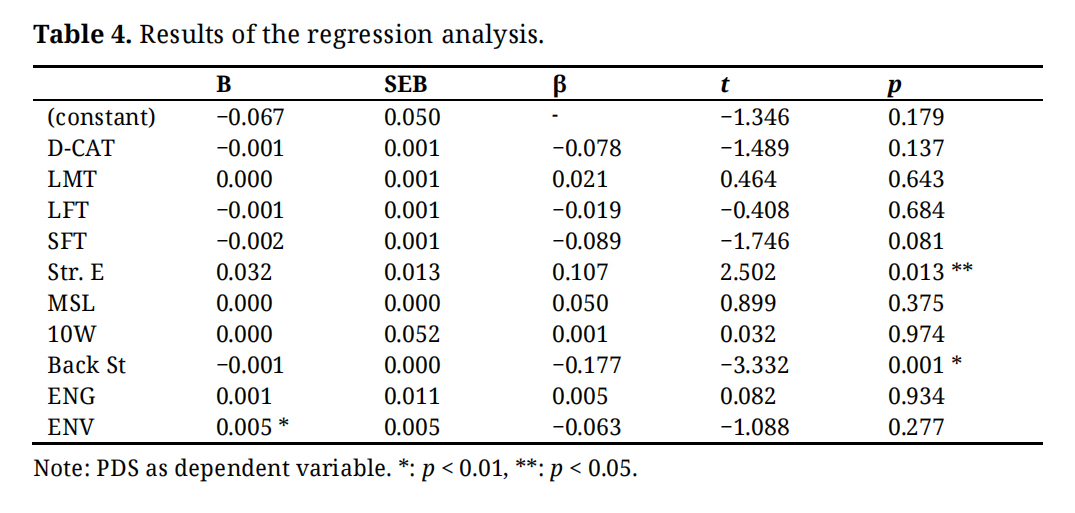 Table 4. Results of the regression analysis.
Table 4. Results of the regression analysis.
The present study investigated the relationship between subjective age and health-related variables (Study 1), and subsequently explored cognitive and physical predictors of subjective age perception (Study 2) among middle-aged and older adults.
Study 1 verified that a younger subjective age is associated with better self-perceived health and vitality, suggesting that individuals who feel younger than their chronological age tend to experience a higher overall sense of well-being. These findings are consistent with previous research indicating that a younger subjective age is linked to more favorable health behaviors, reduced medical service utilization, and greater resilience to chronic pain [9,35]. Moreover, they support the notion that subjective youthfulness can be a proxy indicator of psychological and physical well-being. Importantly, this connection implies that promoting a younger subjective age may have practical applications for health promotion efforts, including psychological interventions aimed at enhancing well-being [36,37].
Study 2 extended these findings by examining which specific cognitive and physical functions are most strongly associated with subjective age perception. Unlike many previous studies that examined cognitive or physical factors in isolation, this study used a unified sample to explore both domains simultaneously. Results from multiple regression analyses revealed that only the Stroop effect size (a measure of executive cognitive function) and back muscle strength (a physical indicator of postural and core strength) were significant predictors of PDS). Other variables related to attention, processing speed, and gross motor function did not significantly contribute to subjective age perception once these two predictors were accounted for.
One consideration is that the emergence of only these two predictors may partly reflect multicollinearity among the independent variables. Although each predictor was selected to represent distinct functional domains, some degree of overlap—such as between attention and executive function or between different aspects of motor function—cannot be ruled out. While multicollinearity does not bias the overall model, it may reduce the ability to detect unique contributions of individual predictors. Future research could incorporate techniques such as variance inflation factor (VIF) analysis to better disentangle the interrelationships among predictors.
These findings support the LiFO hypothesis, which posits that higher-order cognitive and physical functions—those acquired later in human development—are more vulnerable to age-related decline and, crucially, more salient in individuals’ self-assessment of aging. In this view, executive functioning and back muscle strength serve as core referents when individuals evaluate their subjective youthfulness, likely because their deterioration is more noticeable in daily life and more closely tied to one’s sense of autonomy and control.
The distinction between “automatic” versus “controlled” processes may further explain why some physical variables (e.g., walking speed, balance) were not significantly related to subjective age. Tasks like walking or standing are relatively automatic, whereas maintaining posture or engaging the core muscles requires greater conscious effort and control. Similarly, the Stroop test requires inhibition and mental flexibility—hallmarks of executive functioning—indicating that subjective age reflects not merely perceived decline but also an implicit evaluation of one's capacity for self-regulation and agency.
Taken together, these findings provide a dual insight: (1) feeling younger is not only psychologically beneficial but may also reflect an implicit awareness of preserved higher-order functioning; and (2) targeted interventions to maintain back muscle strength and executive functioning may support the maintenance of a younger subjective age. However, as this study is observational and correlational in nature, the directionality of these associations cannot be determined with certainty. It is also possible that better objective health status or lower disease burden may simultaneously contribute to both a younger subjective age and higher quality of life. These alternative explanations should be considered, and future longitudinal or interventional studies are warranted to clarify causal relationships.
Community health programs might nonetheless benefit from incorporating exercises that emphasize core strength, posture awareness, and dual-task training to simultaneously stimulate physical and cognitive systems. While such strategies may support both physical health and the psychological self-concept of aging, these implications should be interpreted with caution given the study’s limitations.
From a public health perspective, reframing aging-related messaging is also warranted. Traditional approaches often emphasize preventing cognitive decline (“don’t get demented”), which may inadvertently reinforce negative age stereotypes. Instead, promoting a positive subjective age—“feel younger, feel healthier”—could enhance older adults’ motivation to engage in health-promoting behaviors and reduce long-term healthcare costs.
Perspectives from cultural neuroscience suggest that cultural differences significantly influence the psychological processes mediated by the brain [38–45]. These cultural influences are likely to be even more pronounced among older adults due to the cumulative nature of sociocultural experiences over the life course. Given that the majority of participants in the present study were born and raised in non-Western societies, caution is warranted when generalizing the findings as universal developmental characteristics of older adults.
Specifically, the participants in this study were residents of Yakumo Town, a rural area in Japan with a high proportion of individuals engaged in agriculture, fishing, and dairy farming. It is plausible that such occupations, which are closely linked to physical labor, may have influenced participants’ assessments of their subjective age. Therefore, the rural and occupational context of the study population should be considered when interpreting the findings.
Recent research [46] has highlighted regional differences in subjective age by comparing rural and urban populations. The study found that both mean subjective age are similar but subjective age among urban residents followed a roughly normal distribution centered around the mean, whereas rural residents exhibited a bimodal distribution, with peaks at both younger and older ends. The bimodal distribution of subjective age among elderly individuals in rural areas is thought to reflect two main factors: their perception of their own physical capabilities in farming and fishing, and their adaptability to operating evolving agricultural machinery. If their work tasks remain similar to those they performed when younger, or if they have successfully adapted to the use of modern machinery, they may perceive themselves as significantly younger. Conversely, those who struggle with physical demands or technological adaptation may perceive themselves as significantly older. These findings underscore the importance of examining subjective age across diverse population samples. Although individuals with orthopedic conditions were excluded from the current study, a more detailed assessment of both physical and mental health—variables known to influence subjective age—remains a methodological challenge and should be addressed in future research.
The present findings indicate that a younger subjective age is closely aligned with perceptions of better health status. Furthermore, declines in higher-order cognitive and physical functions were found to be particularly sensitive to subjective age, lending empirical support to the developmental hypothesis that functions acquired later in life are more susceptible to early deterioration during the aging process. From the standpoint of positive psychology, these results suggest that interventions aimed at preserving or enhancing higher-order functional capacities may be effective in promoting a younger subjective age among older adults. Accordingly, community health practitioners should consider incorporating strategies that support higher-order functioning into programs designed to foster positive aging perceptions.
The authors confirm that they followed professional ethical guidelines in preparing this work. These guidelines include obtaining informed consent from human participants, maintaining ethical treatment and respect for the rights of human or animal participants, and ensuring the privacy of participants and their data, such as ensuring that individual participants cannot be identified in reported results or from publicly available original or archival data. Ethical approval was obtained from the Ethical Committee of Nagoya University Medical School for Yakumo Study (Genetic polymorphism study for resident health examination examinees in Yakumo town; 2011 #643), and written informed consent for participation and data publication was obtained from each participant.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The data of this study is available from the first author based upon reasonable request.
Conceptualization, TH (Takeshi Hatta), YH, AI; data collection, JH, TH (Taketoshi Hatta), MH (Horii Mariko), KK (Kato Kimiko), TK, TH (Takeshi Hatta) AI; statistical analysis, TH (Taketoshi Hatta); writing and editing, TH (Takeshi Hatta), TK, KK; funding acquisition, TH (Takeshi Hatta), TH (Taketoshi Hatta), TK.
Each author signed a form to disclose of potential conflicts of interest. No authors have reported any financial or other conflicts of interest related to the work described.
This study was supported by Grants-in-Aid for Scientific Research (JSPS Grant Nos. 19K11702) and #20K03423 TH (Taketoshi Hatta) #21K04572 TH (Taketoshi Hatta) and #122K09388 TK.
Present authors are indebted to all participants, health management staffs of Yakumo Town and members of the neuropsychology team (Ito Emi, Nagahara Naoko, Fujiwara Kazumi, and Hotta Chie). The authors are also deeply indebted to Richard Harding and Ayano Sasaki-Crawley for their careful advice and editing the English text.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
Hatta T, Hatta T, Horii M, Kimura T, Kato K, Hatta J, et al. Effects of cognitive and physical performances on subjective age perception among community-dwelling older people: Evidence from the yakumo study. Adv Geriatr Med Res. 2025;7(3):e250015. https://doi.org/10.20900/agmr20250015.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




