Location: Home >> Detail
Adv Geriatr Med Res. 2026;8(1):e260004. https://doi.org/10.20900/agmr20260004
 ,
Simona Hapca 2 ,
Dave Hunt 3
,
Simona Hapca 2 ,
Dave Hunt 3
1 Faculty of Health Sciences and Sport, University of Stirling, Stirling FK9 4LA, UK
2 Faculty of Natural Sciences, University of Stirling, Stirling FK9 4LA, UK
3 Noodle-NE Ltd., England DH9 9DB, UK
* Correspondence: Anna C. Whittaker
Background: Physical activity is an important strategy for improving health and quality of life among older adults living in residential care. Less is known about digital physical activity interventions, or their impact on care staff as well as residents. This paper reports on an evaluation of a 12-month scale-up and roll-out of a digital music and movement platform (danceSing Care) across all health boards in Scotland. Methods: Participation during the year of monitoring was between 56-78 care homes at any one time. An online survey incorporating validated measures was used to measure fear of falling, loneliness, and number of sit-to-stands achieved in 30 s in residents and wellbeing, stress and danceSing Care-related job satisfaction among staff at the start of the project, 6 and 12-months. Results: Analyses revealed significant improvements over time for residents’ fear of falling, loneliness, and staff wellbeing, perceived stress and job satisfaction scores. In residents who provided data at multiple times there was also some evidence of an improvement in sit-to-stands. Conclusion: This evaluation provides preliminary evidence that delivering the digital danceSing Care music and movement resources in care homes contributes to improved wellbeing metrics for care home staff and residents but should be taken with caution due to the limitations of the design. A cluster-randomised controlled trial capturing a broader range of health and wellbeing measures in staff and residents would help to confirm these indicative findings.
Residential care homes or homes for the aged face increased pressure due to the ageing of the population globally [1,2], such that many residents are older, frailer [3], and have more long-term health conditions, including dementia, than in previous decades [4]. Consequences of this are reduced quality of life and polypharmacy [5], plus additional burden for care staff looking after a population with increasing needs [6].
Physical activity (PA) interventions can be an effective means to improve health and quality of life in older adults [7]. This is evidenced by positive effects on physical function, such as gait speed, balance and performance in activities of daily living [8], and cognitive function [9] and mental well-being [10], such as anxiety [11]. Dance-based PA interventions have been a particular focus in research due to the socializing and reminiscence opportunities they provide, and benefits demonstrated for wellbeing among older adults generally [12]. For older people in residential care homes, including with dementia, improvements have been demonstrated for mood, cognitive function, social connectedness, mobility and balance [13]. Although many intervention studies focus on resident outcomes rather than the broader social and environmental context [14], some have also shown positive effects on care staff who were empowered to deliver such interventions, resulting in more positive interactions with residents and increased job satisfaction [13].
Recent technological developments and an increase in the proportion of older people using technology [15] have meant that many exercise and dance therapy providers have turned to digital resources to deliver PA interventions. This can also be more accessible and cost-effective for both exercise providers and care homes. Systematic reviews have shown that digital resources to promote PA in older adults in residential care across a range of cognitive and functional ability are feasible and well accepted [16,17]. In a recent study, for older adults’ physical function and fitness, there was no significant difference between online versus in-person exercise classes [18]. However, effects on psychosocial outcomes may differ. Reviews suggest more research into the factors surrounding the successful uptake of such interventions, and accurate measures of effectiveness are needed [16].
danceSing Care (https://dancesing.online) was founded in 2016, transferring traditional exercise and fitness classes into the digital domain. It comprises a set of resources in an online web-based platform with 24/7 access for use by care home staff, e.g., care workers, activity coordinators, with residents. It is a combination of a digital intervention and group-based physical activity program delivered in-person. It was developed specifically for hybrid delivery. Specifically, the exercises were recorded online but the intention from the start was for group in-person delivery using the resource as the guide for this. It consisted of pre-recorded sessions of around 20 min with associated training for care staff and activity coordinators so that they could deliver the sessions in person in a group in the care home with the support of the online videos. Each PA session starts with warm-up activities and ends with cool down activities. The actual PA delivered can be selected by care staff delivering the session, and they can choose from a growing range of activities from yoga to strength and balance work to different dance styles such as salsa and ballroom. The platform includes chair-based and standing exercise to music with the potential to individually tailor movements to ability, focusing on flexibility, strength, balance, and confidence through dance and music. This adds several unique features beyond online or in-person delivery only. First, it means care homes can access evidence-based resources developed specifically for older adults focusing on a range of different types of physical activity which are added to and updated continually, without needing to be physical activity experts themselves. Second, it means care homes can access the resource whenever they wish, without needing to fit around the schedule of an in-person physical activity class leader, and residents can even use it within their own rooms if they do not always feel like joining in a group. Third, the program includes digital support and staff training to facilitate effective use of the resource. This ensures that care homes can address practical issues, such as Wi-Fi connectivity, as well as build staff confidence in delivering safe and enjoyable exercise sessions for older people across a range of abilities. Training also covers how to adapt movements to suit different functional levels.
The theoretical rationale for expecting positive effects of this digital music and movement intervention is several-fold through mechanisms such as increasing physical activity levels, being less sedentary, building strength, and supporting social engagement. Briefly, increasing PA, particularly among those who are mainly sedentary or only engage in low levels of PA, should yield health improvements [19] and aiming to meet the strength and balance guidelines are particularly important for health outcomes in older adults [20]. Second, engaging in PA as a group should increase social cohesion among older adults [21] and thus improve perceived social support and reduce loneliness in older adults as demonstrated previously [22]. Finally, engaging in PA designed specifically to help older adults increase their range of movement was also expected to have benefits on self-confidence in standing and walking and activities of daily living, by building strength and thus reducing fear of falling [23]. However, most of the existing research has been concerned with adults living in the community. Anecdotally, care home staff have reported that the meaningful moments engaged with others while using the programme is as important as the direct benefits of PA and/or music.
In collaboration with danceSing Care we have conducted small-scale studies examining the feasibility, acceptability, and effectiveness of their digital music and movement technology. A mixed methods feasibility study aimed to implement use of the programme 4 times per week (3 movement and music plus 1 music only session) across 10 care homes for 12 weeks [24]. It showed that it was possible to implement the platform within care homes, but the challenges of staff continuity, other priorities due to low staffing (the project was conducted during the Covid pandemic) and Wi-Fi connectivity, meant that delivery at the full recommended dose was challenging with care homes delivering only 57% of the recommended number of sessions, and resident adherence at 60%. Based on staff focus group feedback, recommendations for future implementation included adapting the dose recommendation to 3 sessions per week. Despite considerable changes in staffing and in the cognitive function of resident participants, the preliminary data showed quantitative improvements in anxiety, depression, loneliness, perceived stress and sleep quality. Staff also reported observing improved mood, physical health, social support and job satisfaction in focus groups [24].
A follow-on mixed-methods pilot study prescribed a dose of 2 movement and music and 1 music session per week for 12 weeks using danceSing Care [25]. With this lower dose and emergence from the pandemic, intervention fidelity improved with 88% of prescribed sessions being delivered by staff and attendance by residents at 72%. There were positive effects for residents’ fear of falling, anxiety, loneliness, and salivary DHEA (a hormone related to healthy aging and immune function [26,27], although physical function did not change [25]. More intensive exercise focusing on strength may be needed to produce larger changes in muscle and bone strength and function and reverse age-related decline [28]. Again, although challenges in delivering the intervention in the care home setting were identified, staff and residents also gave positive feedback about the enjoyment and opportunities for reminiscence and social activity that integrating the platform provided, as well as perceived benefits for strength and being less sedentary.
Simultaneously, the Generating Older Active Lives Digitally (GOALD) project was run by the universities of Stirling and Plymouth to explore the impact of digital technology for older people on physical activity, social connectedness and reminiscence. The project trialed and evaluated technologies with older people in community groups and care homes, resulting in a set of co-produced recommendations for technology developers to consider when designing technology specifically aimed at older people [29]. This resulted in a project toolkit which was tested with several technology companies including danceSing. danceSing updated their product interface to be more user friendly and personalized for care organizations, better tailored to and inclusive of older people’s preferences by including them in the video resources, and increasing the variety of resources available plus improved staff resources and support. Several research gaps still remained in the existing research. These include the impact on staff and the longer-term impact on physical function in residents. Effects on staff had only been collected as brief qualitative data from comments made in focus groups by staff in the feasibility and pilot studies. To address this gap in terms of staff impact there was a need to more comprehensively and quantitatively assess the health and wellbeing impact that the intervention might have for care staff delivering it. The previous feasibility and pilot 12-week interventions had not shown evidence of improved physical function e.g., changes in frailty scores, walking speed, balance, in older adults; this might have been due to low power, relatively low intensity of the intervention, or the need to assess these over a longer time frame to see change. To address this gap, we included in our study a measure of physical function at baseline, 6- and 12-months into usage of the intervention.
The Scottish Government Digital Directorate became aware of danceSing and commissioned a 12-month scale-up and roll-out plus light touch evaluation. The aim of the project was to roll-out the platform as a means for care homes to access digital health support to enhance physical activity engagement in care homes, and to evaluate the effects of this. Evaluation of the project was necessarily small-scale due to budget constraints, so was not set up as a research study. Rather, outcome measures were captured mainly by survey run with and by care home staff focusing on mental and social health and physical function of residents plus wellbeing and job satisfaction in staff. Although the evaluation was not explicitly set up to test hypotheses, it was expected that there would be improvements in all these measures.
Participants were residents and care or activities staff from care homes recruited across Scotland who were given up to 12 m free access to danceSing Care. Use of the resource was prescribed based on our previous research, as three sessions to include two music and movement and one music only session per week. This was deemed feasible by care homes, but homes were permitted to vary this to fit within their own schedules and staffing. Participation was voluntary and provided in response to a request to complete periodical evaluation surveys by danceSing. During the project, homes were recruited across all 14 regional NHS Boards. While some care homes left the project, additional care homes were included as the project evolved. Survey data were matched across different time points by name then anonymised before providing to the University of Stirling for secondary data analysis as independent assurance with approval provided by the Stirling General University Ethics Panel (GUEP EC 2025 22360 18594).
MeasuresMeasures were influenced by several criteria including the desire to use industry recognized and validated measures where possible and the need to ensure that the measures were appropriate to the danceSing service. The survey was purposefully kept short to encourage participation and prevent ‘survey fatigue’. Age and sex information were collected from the residents within the survey.
The primary and secondary outcomes were identified in consultation with danceSing and the Scottish Government Digital Directorate team who met several times working as an advisory group to determine appropriate outcomes. The primary outcomes were determined as the resident outcomes in terms of wellbeing and physical function. Research cited above suggests PA interventions can improve these outcomes in this population and particularly dance-based PA in a group setting. The advisory group wished to replicate our previous findings for psychosocial effects but over a longer time frame and at scale. As such, fear of falling and loneliness were chosen as direct replication. Physical function was also determined as a key longer-term primary outcome that should be amenable to change due to the balance and strength work involved in the PA delivered as part of danceSing. However, it was not deemed within the scope of the evaluation to conduct comprehensive batteries of physical function tests validated in geriatric populations via a team of research assistants. After discussion, an alternative commonly-used physical function measure (30 s sit-to-stand) was selected as a brief yet useful proxy of leg strength, feasible for individual care homes to implement themselves with brief video instruction and to capture in the same survey site as fear of falling and loneliness data on residents. The staff outcomes were the secondary outcomes of interest but determined similarly via the team meetings. Measures of staff wellbeing had not been captured comprehensively previously linked to use of danceSing, so wellbeing using a brief validated measure was included as a key outcome. In addition, given the burden on care staff, the team had the perception that providing digital resources to support staff would improve their self-confidence in delivering physical activity and related music activities and this would have knock-on effects on perceptions about their job role. In order to minimize further burden, the survey was kept brief by including a brief stress measure. In the absence of a brief job satisfaction scale suitable to directly assess the impact of using the resource, the team also devised direct questions to measure this. The specific measures are detailed below.
The Falls Efficacy Scale-I short validated in older adults (Cronbach’s alpha = 0.92) measured fear of falling while carrying out daily activities such as getting dressed or attending social events [30]. It is a 7-item scale with responses on a Likert scale from 1–4 (not at all concerned to very much concerned). In the present study, internal consistency was 0.91. The short-form UCLA loneliness scale validated in older adults [31] measured feelings of loneliness among participants. It is composed of 6 items and response options on a 4-point scale (1-never to 4-often), where a high score shows increased feelings of loneliness. Here the internal consistency alpha was 0.84. For pragmatic reasons, assessment of physical function was limited to measuring sit-to-stands in 30 seconds which is a proxy for leg strength and endurance [32]. Residents stand unaided from a sitting position as many times as possible in 30 s.
Staff were surveyed using three questionnaires. Wellbeing was assessed using the Warwick-Edinburgh Mental Well-Being Scale [33] which consists of 14 items about feelings and thoughts in the last two weeks with responses from 1-none of the time to 5- all of the time. Internal consistency was 0.92. Perceived stress was measured using the 10-item Perceived Stress Scale [34] where questions assess how often they felt a certain way in the past month on a 5-point scale from 0-never to ‘4- very often. Cronbach’s alpha for the scale was 0.84. Job satisfaction was assessed through 7 questions specifically devised to apply to danceSing Care. These included statements about the perceived positive impact of their work, appreciation by residents and their families, recognition by their organization, whether they got the training they needed to use the resource, whether they enjoyed using it, and understood the potential benefits of it, and whether it had improved their relationship with residents. These were scored from 0-strongly disagree to 4-strongly agree and were summed to provide an overall score.
ProcedureThe survey was distributed electronically to staff at each care home via a QR code to complete themselves and to distribute to residents to complete, or to support residents or their families to complete it. When the survey was not completed by the resident themselves, it was noted whether the person completing it did so with the resident’s participation or about the resident. Although this recruitment strategy was directed to all staff as an attempt to also recruit all residents where possible, it was not possible to monitor this and participation was voluntary. Email recruitment was followed up with regular reminders at in–person training and catch-up sessions with staff. The initial survey phase was between October 2023 and January 2024. The survey was circulated again 6 and 12 months after the initial phase, between March and June 2024, then September and October 2024. The intention was to capture repeated measures as much and as far as possible, although with different homes joining and leaving the project at different points, it was not possible to fully control this. Following initial in-person training of staff with the resources, additional training and catch-up sessions were provided throughout 2024 to onboard new care homes and support continued engagement. These sessions were delivered as a flexible mix of in-person visits to individual care homes and online sessions to accommodate varying schedules. The catch-up or ‘connect and reflect’ sessions were run online to foster a sense of community within danceSing, and to gather feedback from staff. These meetings also included reporting on average usage of the danceSing platform per month across homes to motivate use. Notes and transcriptions (where possible) from the meetings were archived in the University of Stirling’s data repository and are available upon request.
Data AnalysisContinuity of data collection across staff and residents was challenging as different care homes were joining and leaving the project in different months and some of the care homes did not fully understand the need for completion more than once despite the initial briefing and reminders. To manage missing data but conduct an analysis of a time effect across the survey points, Linear Mixed Effect Models were run with questionnaire or sit-to-stand totals as separate dependent variables and time (baseline, 6 m, 12 m) as the fixed factor and staff or resident ID number as the random factor. For resident outcome measures, effects of age and sex were also tested and added to adjusted models as fixed factors. Alpha was set at p = 0.05 to indicate statistical significance.
The project commenced in November 2023 with 65 homes taking part and ended in October 2024 with 68 homes participating; a total of 78 homes participated at some point during the project, with 56 taking part the whole of the year. Separate analysis of usage of the platform by danceSing showed that at month one the average hours per month used per home was 2.5 which would equate to 1.9 × 20-minute sessions per week. By month three the platform was sufficiently used on average equating to the prescribed three sessions per week and in month eight usage was 13.7 h per month per home equating to about 10.2 sessions per week. Part-way through the project, the Scottish Government Team suggested that homes be asked to use the program for at least five hours per month; this was achieved across all homes by month eight and was maintained until the end of the project. Average engagement hours across homes are shown in Figure 1.
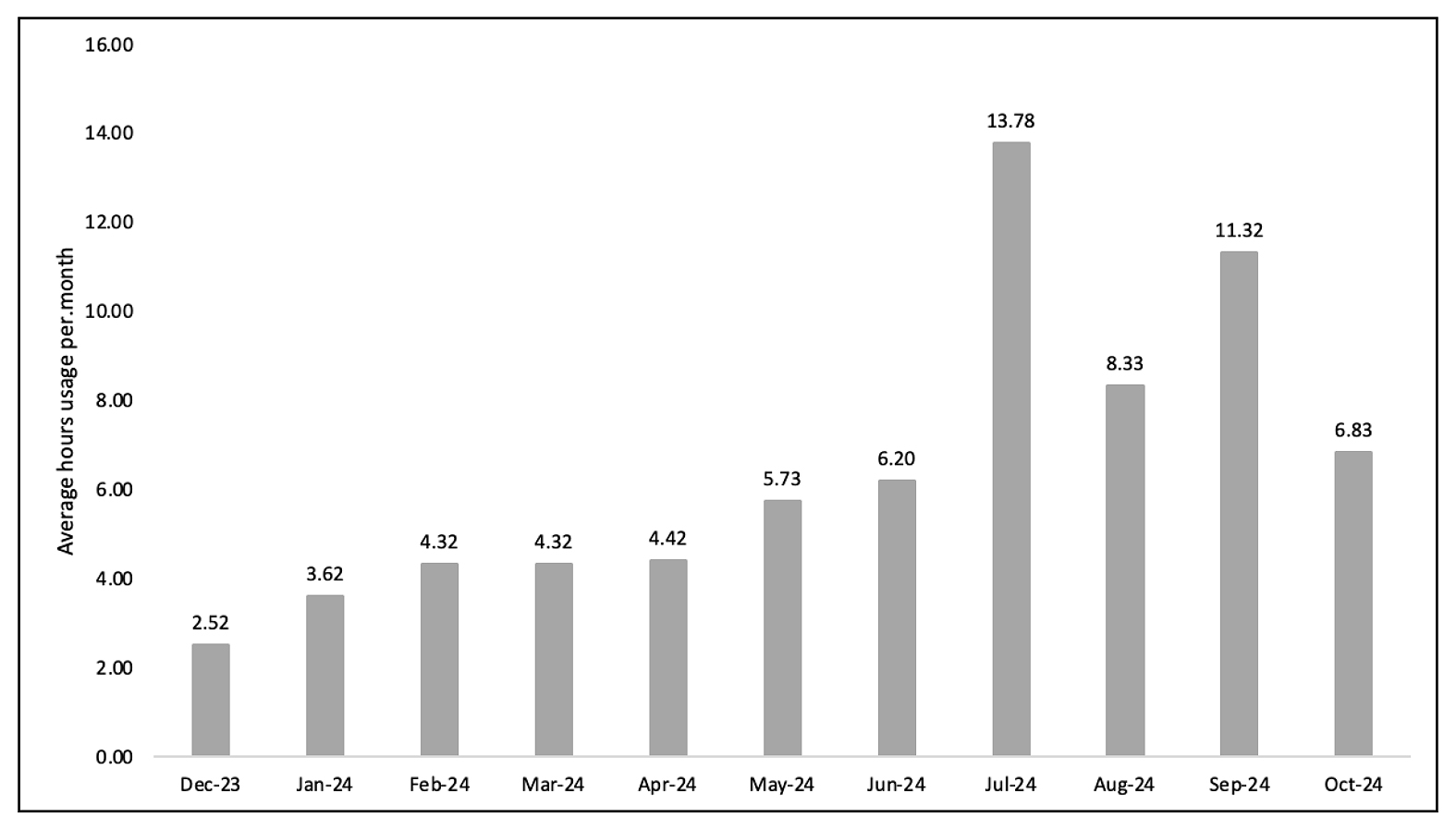 Figure 1. Mean hours use of the platform across all homes using it per month.
Figure 1. Mean hours use of the platform across all homes using it per month.
The numbers of survey responses separately by resident participants and staff participants at each time point and descriptive statistics are shown in Table 1. Twenty-nine specific residents took part at Time 1 only, 24 at Time 2 only, and 48 at Time 3 only; this meant that 35 contributed data twice. Of the staff, 68 participated at Time 1 only, 21 at Time 2 only, and 17 at Time 3 only, meaning that 26 staff provided data twice. No residents or staff took part at all three timepoints. The changes in age are due to different homes entering and leaving the evaluation at different time points as the year went on, as well as residents entering and leaving homes, hence at time 2, only 44% were aged 75-90 years whereas at baseline this was 78%.
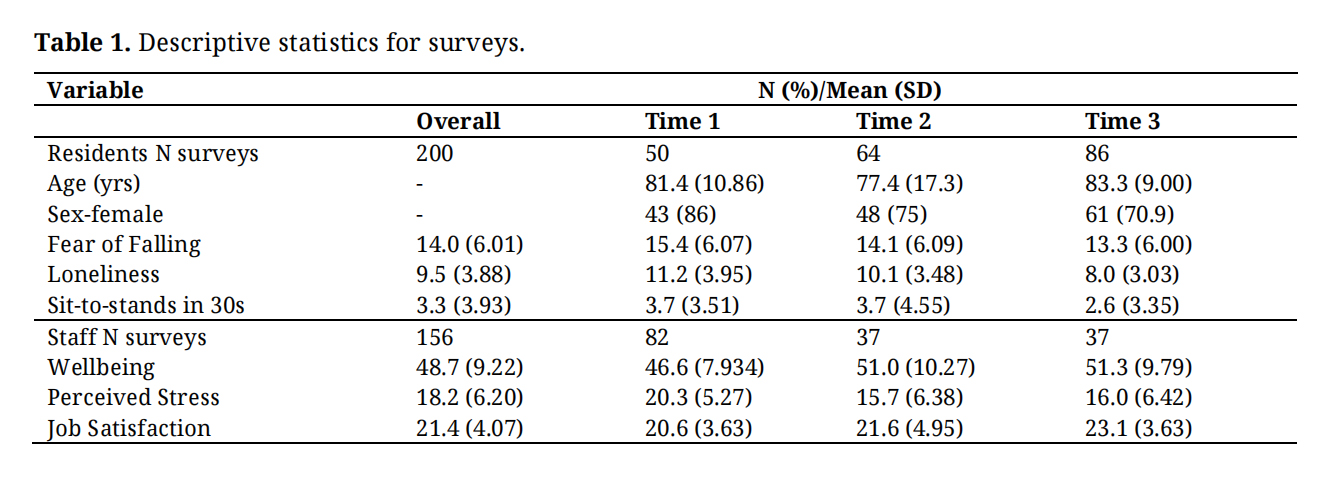 Table 1. Descriptive statistics for surveys.
Table 1. Descriptive statistics for surveys.
For residents, linear mixed models with adjustment for age and sex revealed a significant main effect of time for fear of falling (F(2, 84.7) = 4.05, p = 0.02), with significant differences revealed between baseline (the referent category) and 12 months but not between baseline and 6 months, such that over the year fear of falling declined 13.6% between the average at baseline to the end of the project; there was no significant effect of sex but as age increased so did fear of falling. There was a main effect of time for loneliness (F(2, 158.4) = 10.42, p < 0.001) with significant differences between baseline and 12 months, but not quite significant between baseline and 6 months, such that loneliness significantly declined 29.1% over the year; pairwise comparisons showed loneliness was also significantly lower at 12m compared to 6m (p = 0.006), but there was no significant effect of age or sex. There was no overall effect of time for sit-to-stands (F(2, 102.7) = 0.49, p = 0.62) or between baseline and either 6 or 12 months. Analysis of the participants (n = 15) who provided data on sit-to-stands at both the mid-point and final survey showed that these increased by 29%. Coefficients are shown in Table 2 and effects are displayed in Figure 2. There was no significant effect of sex on sit-to-stands but as age increased, sit-to-stands number significantly decreased.
For staff, Linear Mixed models revealed significant effects of time for wellbeing (F(2, 75.3) = 4.13, p = 0.02), perceived stress (F(2, 83.9) = 10.31, p < 0.001) and job satisfaction (F(2, 126.1) = 5.31, p = 0.006). For wellbeing and stress, improvements were evident between baseline and both 6 and 12 months representing an overall 10.2% improvement in wellbeing and 21.2% decrease in stress between baseline and 12 months (see Figure 1). For job satisfaction, the significant difference was between baseline and 12 months only (see Table 2), representing an overall improvement of 12.4%.
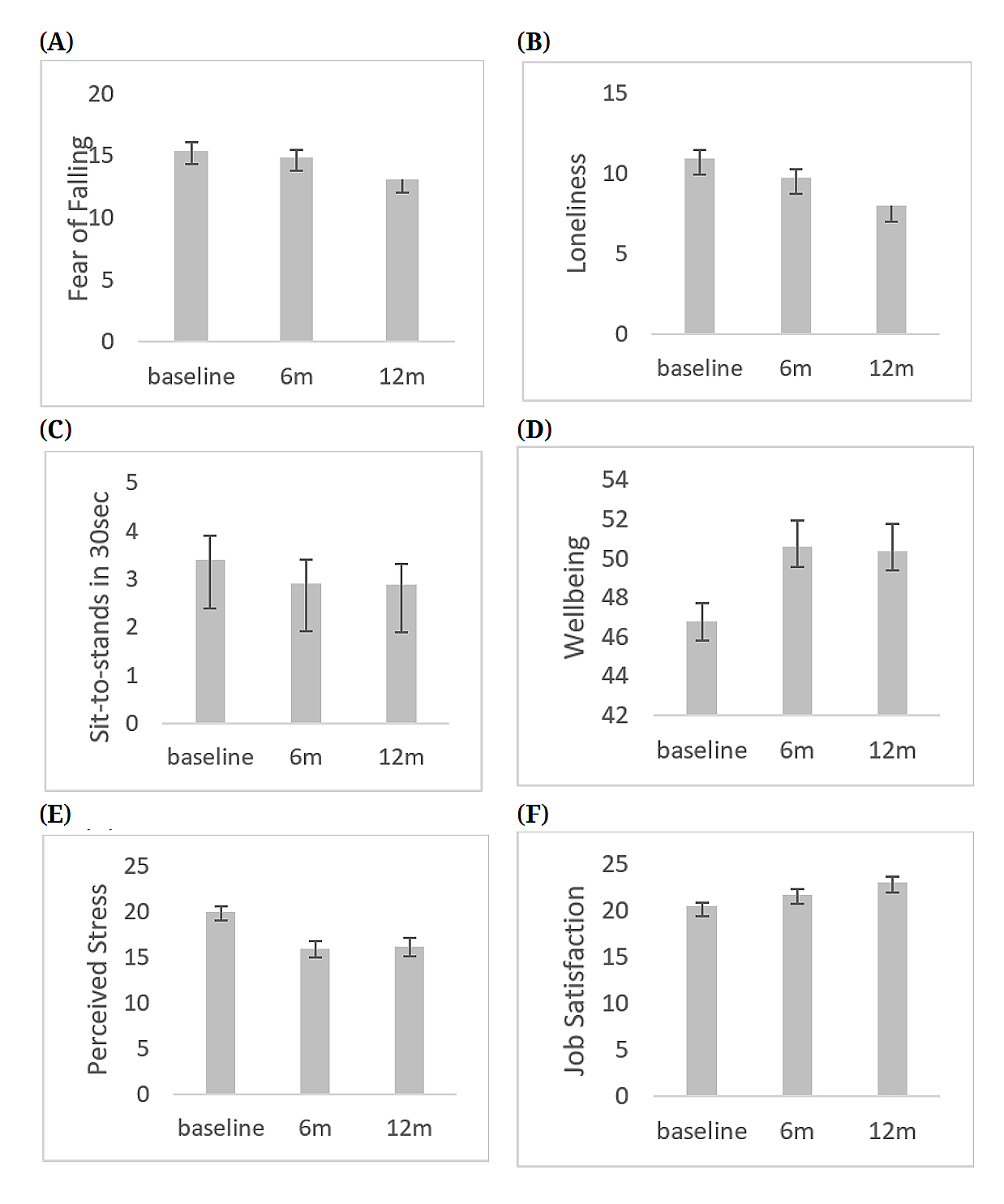 Figure 2. Mean (SE) scores across participants at each time point (A) Fear of Falling. (B) Loneliness. (C) Sit-to-stands in 30 s. (D) Wellbeing. (E) Perceived Stress. (F) Job satisfaction.
Figure 2. Mean (SE) scores across participants at each time point (A) Fear of Falling. (B) Loneliness. (C) Sit-to-stands in 30 s. (D) Wellbeing. (E) Perceived Stress. (F) Job satisfaction.
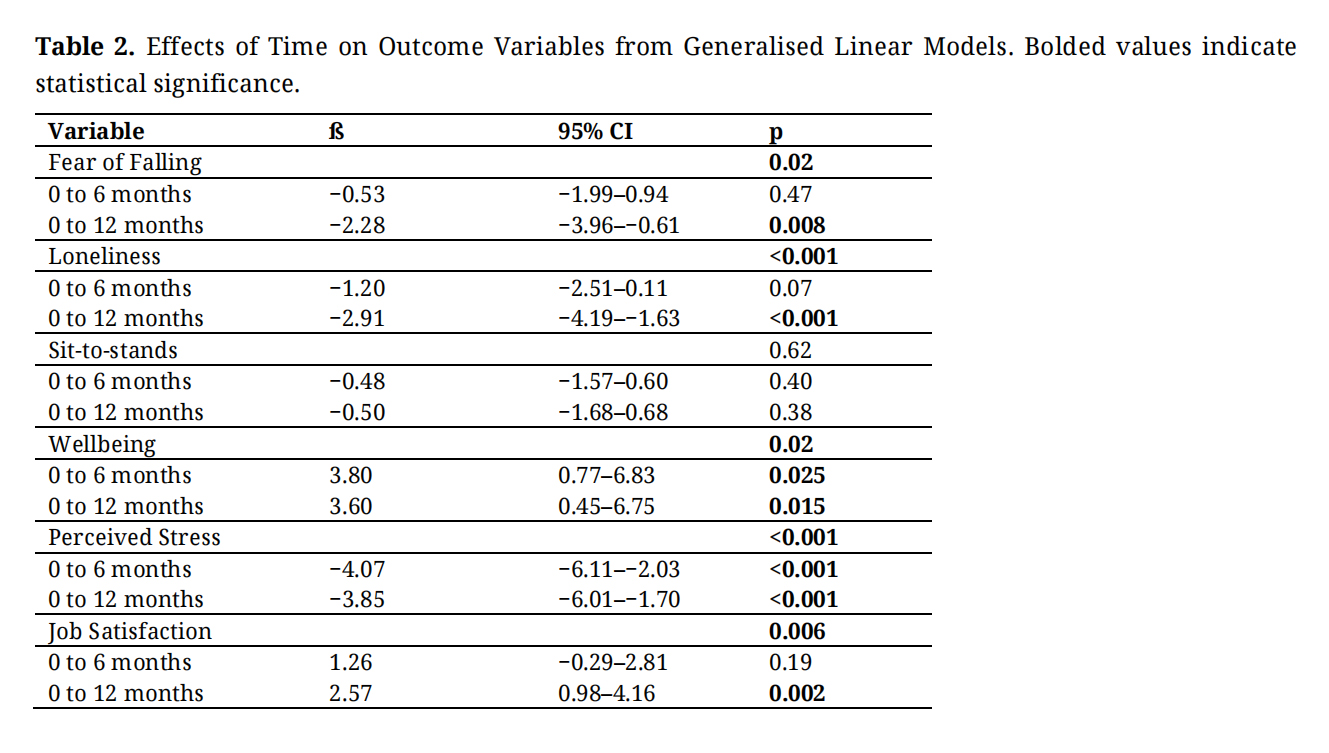 Table 2. Effects of Time on Outcome Variables from Generalised Linear Models. Bolded values indicate statistical significance.
Table 2. Effects of Time on Outcome Variables from Generalised Linear Models. Bolded values indicate statistical significance.
This light-touch evaluation of the impact of using the danceSing Care platform over the course of one year revealed improvements in fear of falling and loneliness among older adult care home residents, and improvements in wellbeing, perceived stress levels and job satisfaction among staff. Findings should be interpreted as preliminary and with caution due to the limitations of the design, discussed below.
These findings are broadly in line with those of our previous small-scale research studies which showed positive effects for residents’ loneliness [18,19], and fear of falling [25], but not physical function across 12-weeks of use of the programme. This also corresponded with the mixed evidence for the effectiveness for digital interventions for increasing physical activity and improving physical function with the main positive effects being for neuropsychiatric symptoms such as depression [16].
Improving a sense of community is one mechanism by which interventions can improve loneliness and therefore quality of life in older adults [35]. However, earlier systematic reviews of physical activity interventions for social outcomes including loneliness have not always shown conclusive results [36]. Consequently, this evaluation adds to the growing evidence that group-based physical activity can be beneficial for this outcome due to providing social elements within the intervention delivery [27]. This evaluation also shows that loneliness can be improved with the support of digital technology, which might seem counter-intuitive, but it is worth noting that the technology here is delivered online but with crucial in-person support of care staff in a group setting within care homes, thus contributes to opportunities for residents and staff to engage in meaningful activity together. Indeed, comments from ‘connect and reflect’ sessions with staff during the year revealed they had observed significant boosts to social connection, reduced loneliness, and improved staff and resident morale.
Previous research including our own has not consistently shown improvements in fear of falling measured through falls efficacy scales [16], but the present evaluation adds to the growing evidence of significant improvements over time. It is possible that by participating in activities in the platform designed to improve strength and balance, which should therefore increase self-confidence in standing and walking would thus reduce the fear of falling [23]. Many of the previous studies reviewed in this area focused on exergaming rather than dance or similar music and movement interventions, so may differ in terms of the outcomes they are specifically targeting for improvement, and therefore the effects demonstrated. As fear of falling can lead to avoiding physical activity, decreasing this fear should result in more confidence in moving, increased activity and thereby improved physical function. However, it should also be noted that our recruitment approach may have been affected by selection bias, as it is possible that residents who volunteered to take part in the survey were also those who already felt more positive about the program. Improved fear of falling might also reflect other changes in the care homes’ environment, e.g., improved lighting or flooring, taking place over the evaluation year which we are unable to account for. However, it is encouraging that these findings are supported by our previous repeated-measures small-scale study [25]. Obviously, a more rigorous randomized controlled design would be necessary to infer causal effects of the program on these outcomes. There is some evidence that the improvements observed in fear of falling do not result in an increased risk of falls [23] and may help prevent falls by increasing activity and improving gait [37]. Future research could assess whether reduced fear of falling translates into fewer falls in the care home setting longitudinally.
The lack of significant effect on sit-to-stands as a proxy measure of leg strength in this study is likely due to the aging of the population completing the evaluation survey across the year. The improvements among the participants who completed repeated measures is encouraging but should be considered tentative due to the small sample in this sub-group. It is possible that greater improvements would be observed with a larger number of consistent participants contributing to the dataset. However, to exclude practice effects, a no-intervention control group would also need to be tested, which was not possible in this evaluation project. Positively, improvements in sit-to-stands have been shown to translate into improved mobility and function in care home residents [38] so can be a simple yet effective activity as well as important outcome measure in this population.
The present evaluation also demonstrated benefits for staff from this digital physical activity and music intervention. This is in line with our previous studies where qualitative evidence suggested staff enjoyed and benefitted from engaging more with residents in these types of activities [24,25]. Further, discussions with staff during the roll-out revealed qualitative improvements in morale as mentioned above as well as increased suppleness. Many previous interventions do not consider the wider care home context beyond the residents [14]. Where staff views have been considered, this has often been in relation to the benefits and risks to residents themselves of engaging in such activities e.g., [39] but meaningful improvements in psychological wellbeing and caregiving ability have been reported where measured [40]. The benefits of staff feeling more satisfied in their jobs and having better wellbeing is likely to translate into improved care and resident outcomes. The effect of participating in the intervention on staff stress levels is particularly interesting given the high levels of stress among social care staff [41], particularly where nursing care demands, and bed numbers are high [42]. This shows that this type of intervention may be a promising means of improving staff outcomes as well as residents’ and potentially reducing the high staff turnover in this setting.
It is important to note that there are several implementation implications for running this type of program in care homes. First, the cost of subscribing to continued use following the free provision during this evaluation phase. Second, the staff time required to complete training on how to use the program and time to deliver it, particularly in a setting which has high staff turnover. However, there were several observations during this evaluation which suggested that these are surmountable issues. First, after 12-months of this evaluation project, 30 out of 68 homes (49%) engaged in the program had opted to continue and paid to do so, suggesting that they deemed it value for money, cost-effective and sustainable. Second, the qualitative data from the ‘connect and reflect’ sessions showed staff enjoyed engaging with the program and appreciated the additional support and engagement such as the group Facebook pages, suggesting that at least those engaged enough to attend these sessions did not deem it onerous, but beneficial. Again, a more controlled design with repeated measures would be needed to establish this firmly. Anecdotal evidence from discussions with care home management of an organization whose seven homes were part of the project confirmed that they felt that the resource requirements were justified and value for money. These homes have continued to subscribe to the program and contribute to research to support a more rigorous evaluation of impact on the care home environment (Whittaker, 2026, direct communication with Abbotsford Care).
LimitationsGiven this was a small-scale evaluation using secondary data rather than intervention research, there are several limitations which should be considered when drawing conclusions about the effects. First, it was not possible to implement a rigorous repeated-measures design, and the project was not funded as research or to include researcher support for targeted recruitment data collection, so it depended on regular email reminders and online check-in meetings from danceSing to stimulate completion of the surveys. This introduces potential sampling bias and resulted in considerable missing data, including missing repeated measures, as well as relatively low response rates to the surveys although we are unable to directly measure this without knowing the number of residents per home involved, thus analyses to examine overall trends was selected rather than repeated measures. However, the findings reflect what we have demonstrated previously in our smaller scale studies and qualitative data which gives confidence to the present findings in this larger sample.
Second, a randomised controlled design would be the gold standard for substantiating claims of positive effects associated with the use of danceSing Care, by being able to exclude potential confounding effects, as well as to collect data on participation rates per home, fidelity or intensity of the intervention or adherence to the dose frequency prescribed, of the intervention beyond the average hours use per home per month. However, the average usage per month suggests that although homes did not initially engage in the prescribed three sessions per week in the first month, by month three they had reached the prescribed dose for several months. While usage varied over time, the average use exceeded the prescribed dose for several subsequent months. It was not possible to implement a more rigorous design or collect specific participation, adherence, or fidelity data, which means the conclusions drawn here should be taken with caution and future research should look to utilise a stronger design to include collection of this additional information. Previous experience in this setting suggests a cluster-randomised controlled design would be more effective than individual randomisation to intervention or waitlist control groups given the difficulties of excluding residents from ongoing activities in their home. Third, the evaluation was limited to a small number of measures due to the demands of the setting and need to reduce staff and resident burden. However, these were diverse enough to measure different aspects of wellbeing in both residents and staff. The inclusion of both residents and staff was intentional, building on earlier work focused only on residents.
The survey’s simplicity meant we could not collect the additional detail needed for deeper analysis, as funding only supported a brief evaluation that staff and residents could complete within their limited time. Due to resource constraints, physical function was only assessed using sit-to-stands, which of course can only be undertaken by individuals who are able to support themselves in a chair and into a standing position, thus meaning no data on strength are available for residents with a health condition or disability preventing this. However, sit-to-stands are a recognised proxy for strength and balance in older people [11], albeit mainly in community-dwelling adults, and have the advantage of being simple to implement without specialist assistance and provided a snapshot of any improvements in physical function for a proportion of the care home residents involved. Future studies should implement standardised measures of strength, balance, and walking speed to give a fuller picture of functional ability.
Finally, the job satisfaction questions were not based on a psychometric questionnaire but rather were specific to danceSing care which might reduce the validity of the measure, and means that we are unable to report on its psychometric properties including how well it captures job satisfaction relative to concurrent validated scales, however, this provided specific useful feedback to the technology developers and care homes which could then be addressed in ‘connect and reflect’ sessions.
In conclusion, this evaluation provides preliminary evidence that use of the danceSing Care digital platform for music and movement resources and delivery in care homes can contribute to improved wellbeing metrics for both care home staff and residents. Future research should attempt to implement a more rigorous cluster-randomised controlled design and extend to a broader range of health and wellbeing measures in staff and residents, including a more comprehensive assessment of physical function.
The study (secondary data analysis) was approved by University of Stirling general university ethics panel (GUEP EC 2025 22360 18594) 22.10.25. Informed consent was not applicable due to the data not being collected for research purposes but as part of a programme evaluation run by danceSing, however, assent to complete the surveys and discussions was voluntary and implied by completion/attendance and all data provided for secondary analysis were anonymized. Staff/residents who took part in the evaluation were informed that their data would not be identifiable to third parties in any analyses or reports.
Declaration of Helsinki STROBE Reporting GuidelineThe data were collected as part of a programme evaluation rather than as research data so informed consent was not collected. Staff and residents who provided data completed the survey voluntarily as part of the programme evaluation and were informed at this point that it would be anonymised.
Ethics Committee-University of Stirling General University Ethical Panel gave approval for the secondary data analysis for the purposes of this manuscript Ethics Reference Number: (GUEP EC 2025 22360 18594).
The dataset generated analyzed in the study can be found at University of Stirling dataSTORRE https://datastorre.stir.ac.uk/.
Conceptualization, AW, DH; Data curation, AW, DH; Funding acquisition, danceSing, AW; Investigation, danceSing, DH; Methodology, danceSing, AW, SH; Project administration, danceSing, DH; Supervision, AW; Data Analysis; AW, DH, SH; Writing–original draft, AW; Writing–review & editing, AW, SH, DH.
AW provided consultancy on this project, receiving £15,000 (of the grant awarded to danceSing) to the University of Stirling (not personally) to support this activity. DH is an independent programme management consultant but was contracted by danceSing to provide administrative support with data collection, curation, and report writing for the original Scottish government project and received financial support of £11,500. DH declared a close relationship with a member of the danceSing executive.
The Scottish Government Digital Directorate funded the scale-up and roll-out and light touch evaluation awarding £125,000 to danceSing; of this £15,000 to University of Stirling for consultancy on methodology and analysis.
The authors would like to acknowledge: 1) danceSing for providing their platform free of charge for the duration of the project and for utilising the funding to support training for care home staff, catch-up sessions, IT support, and evaluation project implementation; 2) Care homes for being willing to participate in the project and evaluation; these are listed in the Appendix of the full report which can be found here: https://1000elders.stir.ac.uk/2025/03/14/update-on-our-dancesing-care-scottish-government-project/ and 3) Care home staff and residents for participating.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Whittaker AC, Hapca S, Hunt D. Evaluation of the impact of digital music and movement on care home staff and resident outcomes. Adv Geriatr Med Res. 2026;8(1):e260004. https://doi.org/10.20900/agmr20260004

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




